

About the Procedure
Functional septorhinoplasty is surgery of the nose that treats the structures responsible for nasal breathing and, when a patient also wishes it, the external appearance of the nose in the same operation. The "septo" part refers to the nasal septum, the wall of cartilage and bone that divides the two sides of the nose. The "rhino" part refers to the wider nasal framework: the bones at the top, the cartilages that shape the middle and lower nose, the internal and external nasal valves, and the support structures that keep the airway open during normal breathing.
The term is meant to distinguish this operation from two narrower procedures it is often confused with. A septoplasty straightens a deviated septum but does not, by itself, change the external shape of the nose or rebuild a collapsed nasal valve. A purely cosmetic rhinoplasty changes appearance but may not be planned around breathing and, if cartilage is removed without restoring support, can sometimes make breathing worse over time. Functional septorhinoplasty is designed to do both jobs together: improve or preserve the nasal airway while keeping the nose looking natural and balanced.
At Norelle Health in New York City, the operation is planned individually. Some patients come primarily because they cannot breathe well through the nose — they may have a deviated septum, valve collapse, large turbinates, the after-effects of an old injury, or breathing problems that followed a previous nasal surgery. Others come with both a breathing concern and a wish to refine a dorsal hump, a crooked nose, a drooping tip, or asymmetry left by trauma. The goal of the consultation is to identify exactly where the airway is narrowing, decide which structural problems are contributing, and agree on what a realistic, durable result looks like for that person. No two noses are rebuilt the same way, and the right plan depends on the anatomy, the patient's goals, prior surgery, and overall health rather than on the name of the procedure.
How the nose controls breathing
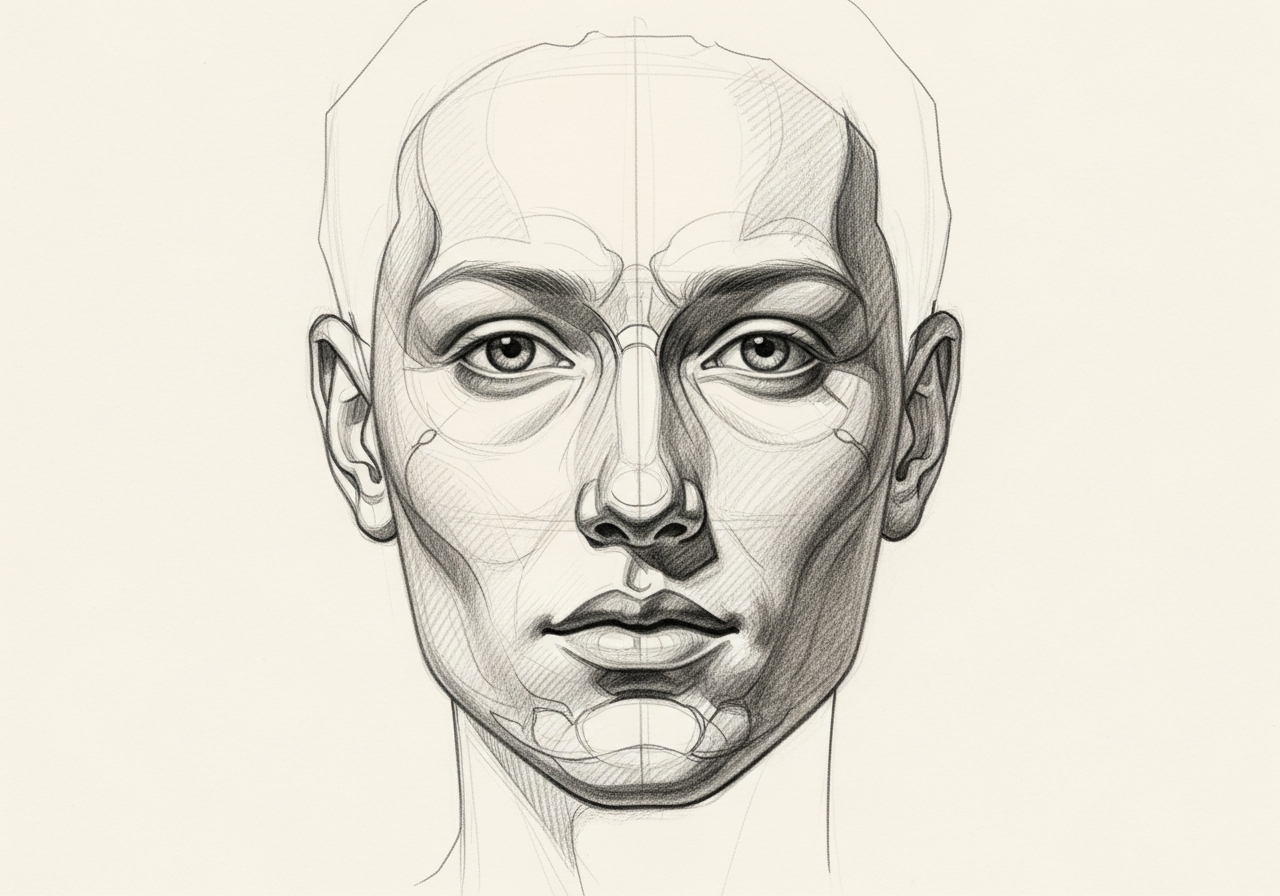
Most people picture the nose as a simple open tube, but airflow through it is controlled by several specific structures, and a problem at any one of them can make the nose feel blocked.
- The septum divides the nasal cavity into a right and left passage. When it is deviated — bent or buckled toward one side — it narrows that passage and disturbs airflow. Septal deviation can be present from birth, develop during growth, or follow an injury.
- The internal nasal valve is the narrowest part of the nasal airway, where the upper cartilage meets the septum partway up the nose. Because it is the tightest point, even small amounts of narrowing or collapse here have an outsized effect on how blocked the nose feels.
- The external nasal valve is the area around the nostril rim, supported by the lower cartilages. When this region is weak — often after aging, prior surgery, or because of naturally thin cartilage — the nostril can draw inward on inspiration, especially with deeper breaths during exercise.
- The turbinates are shelf-like structures on the side walls of the nose that warm and humidify air. When they are chronically enlarged from allergy, irritation, or in response to a deviated septum, they reduce the space available for airflow.
- The cartilage framework as a whole provides the support that holds all of these open. If support is weak or has been over-reduced by previous surgery, the airway can narrow dynamically each time the patient breathes in.
Understanding which of these structures is responsible is the central task of evaluation, because a nose can feel "stuffy" for very different mechanical reasons, and each reason is treated differently.
Considering functional septorhinoplasty? The next step is a quiet, unhurried conversation.
Structural problems this surgery can address
Functional septorhinoplasty is used when nasal obstruction or external nasal deformity is caused by the structure of the nose rather than only by inflammation that medicine can control. Common structural targets include:
- Deviated septum causing persistent obstruction on one or both sides.
- Internal nasal valve narrowing or collapse, frequently the most under-recognized cause of nasal obstruction and a common reason breathing does not improve after a septoplasty alone.
- External nasal valve weakness, where the nostril sidewall collapses inward with breathing.
- Turbinate hypertrophy contributing to airway narrowing alongside structural problems.
- Post-traumatic deformity, such as a crooked or twisted nose, a saddle (collapsed bridge) deformity, or a healed nasal fracture that left both a breathing problem and a visible change.
- Iatrogenic obstruction after previous surgery, where cartilage was removed without adequate support and the airway has narrowed or the bridge and tip have weakened over time.
When a patient also has appearance concerns — a dorsal hump, a wide or asymmetric bridge, a bulbous or drooping tip — those can be addressed in the same operation, planned so that any change to shape does not come at the expense of breathing.
Why function and appearance are planned together
Breathing and appearance are physically linked in the nose, which is why combining them in one well-planned operation often makes sense.
The structures that shape the outside of the nose are the same ones that hold the airway open on the inside. Reducing a dorsal hump, narrowing a wide bridge, or refining a tip all involve adjusting cartilage and bone that also support the internal and external valves. If those changes are made without restoring support — for example, with grafts that reinforce the valve — the nose may look improved at first but breathe worse months or years later. Conversely, straightening a badly deviated, twisted nose to improve airflow usually also straightens its visible appearance.
Planning both together has practical advantages. It means one anesthetic, one recovery period, and one healing process rather than two separate surgeries. It also allows the surgeon to use the patient's own cartilage efficiently — for instance, using septal cartilage both to straighten the septum and to build grafts that support the valves and refine the shape. The alternative, operating twice, adds cost, recovery time, and scarring, and a second operation through previously operated tissue is generally more complex.
This does not mean every patient wants or needs a cosmetic change. Many functional septorhinoplasties are done purely to improve breathing, with no change intended to the external appearance. The point is that the breathing-related work is planned with the appearance in mind, and any appearance-related work is planned with breathing in mind.
How the procedure is performed
Functional septorhinoplasty is highly individualized, but several techniques are commonly combined depending on what the evaluation finds.
Surgical approach. The operation can be performed closed (endonasal), with all incisions hidden inside the nostrils, or open (external), which adds a small incision across the columella — the strip of skin between the nostrils — that usually heals to a faint, well-concealed scar. The open approach gives the surgeon direct visibility and more precise control for complex straightening, grafting, and revision work; the closed approach avoids the external incision and may be appropriate for more limited problems. The choice depends on the anatomy and the goals, not on a single preference.
Septal correction. Deviated cartilage and bone are straightened, repositioned, or selectively removed, while preserving enough septal support to keep the bridge and tip stable. Straight portions of removed septal cartilage are often saved and reshaped into grafts.
Nasal valve repair. Internal valve narrowing is commonly treated with spreader grafts — strips of cartilage placed alongside the septum to widen and reinforce the valve. External valve collapse may be treated with alar batten or rim grafts that strengthen the nostril sidewall so it resists collapsing inward during breathing.
Turbinate reduction. When enlarged turbinates contribute to obstruction, they are reduced in a tissue-preserving way that improves airflow while keeping enough turbinate to warm and humidify air.
Reshaping the framework. When appearance is part of the plan, a dorsal hump may be lowered, the bony bridge narrowed with controlled osteotomies (precise bone repositioning), and the tip cartilages refined and supported. Cartilage grafts — from the septum, and in revision or complex cases from the ear or rib — are used to rebuild support and create a stable, natural shape.
Anesthesia and setting. The operation is typically performed under general anesthesia as an outpatient procedure, meaning most patients go home the same day. Length varies with complexity, commonly ranging from roughly one to several hours. Internal soft splints and/or an external splint are often placed to support healing; many surgeons now avoid traditional packing.

How functional septorhinoplasty differs from related procedures
Several nasal procedures overlap, and choosing among them is part of the evaluation.
- Septoplasty corrects a deviated septum only. It is the right operation when the septum is the sole structural problem and the nasal valves, external shape, and support are otherwise fine. It does not address valve collapse or change appearance.
- Turbinate reduction alone treats enlarged turbinates but does nothing for a deviated septum, valve collapse, or shape. It is often combined with other steps rather than performed in isolation.
- Cosmetic rhinoplasty changes external appearance. When planned without attention to support and the valves, it carries a risk of worsening breathing, which is why functional planning matters even for primarily aesthetic cases.
- Revision rhinoplasty addresses problems remaining after a previous nasal operation. Functional septorhinoplasty principles are central to revision work, because many revisions are needed precisely because support and the valves were not preserved the first time.
Functional septorhinoplasty is most clearly understood as the integrated operation that brings these elements together when more than one structure is involved.
Revision and complex cases
Some patients come after one or more previous nasal operations, with a combination of persistent obstruction and an appearance they are unhappy with. These revision cases are generally more complex than a first-time operation for several reasons: scar tissue distorts the normal tissue planes, native cartilage may have been removed or weakened, and the skin may behave differently after prior surgery.
When the septum no longer provides enough cartilage for grafting, the surgeon may use cartilage from the ear (conchal cartilage) or, for larger structural needs, the rib (costal cartilage). Rib cartilage provides a strong, abundant source for rebuilding a collapsed bridge or major support, with its own set of considerations including a separate small incision and recovery at the donor site.
Revision functional septorhinoplasty often focuses on rebuilding support that was lost — restoring the bridge, reinforcing the valves, and re-establishing tip support — so that the nose both breathes and looks stable over the long term. Because these operations are demanding and the tissue is less forgiving, planning, realistic expectations, and an honest discussion of what can and cannot be improved are especially important.
Risks and important considerations
Like any operation, functional septorhinoplasty has risks, and an informed decision means understanding them. They include:
- Bleeding during or after surgery, usually minor but occasionally requiring treatment.
- Infection, which is uncommon but possible and may require antibiotics.
- Septal perforation — a small hole in the septum — which can occur when working on a thin or previously operated septum and may cause crusting, whistling, or bleeding.
- Residual or recurrent obstruction. Surgery aims to improve breathing, but it cannot guarantee a perfectly clear airway, and some patients have ongoing symptoms from inflammation, allergy, or healing.
- Changes in appearance that may differ from expectations, including asymmetry, irregularities felt or seen along the bridge, or changes that become apparent only as swelling resolves over months.
- Need for revision surgery in a minority of patients, more commonly after complex or revision cases.
- Temporary numbness of the nasal tip or upper front teeth, and changes in the sense of smell, which are usually temporary.
- Anesthesia-related risks, which are discussed separately as part of the surgical consent.
No surgeon can promise a specific cosmetic result or a guaranteed level of breathing improvement. A careful evaluation, realistic goals, and clear communication reduce the chance of disappointment and help align the surgical plan with what matters most to the patient.
Nonsurgical and adjunct options
Surgery is not always the first step. Because nasal obstruction can come from inflammation as well as structure, it is reasonable to treat the reversible causes first and to keep treating them after surgery if they are present.
- Medical management of rhinitis and allergy — nasal steroid sprays, antihistamines, saline irrigation, and, when appropriate, allergy evaluation and immunotherapy — can reduce turbinate swelling and congestion. If allergy is a major driver, surgery on structure alone will not fully solve the problem.
- Treating chronic sinus disease when sinus inflammation is contributing to symptoms.
- External nasal dilator strips or internal nasal dilators can give a temporary sense of how much valve support might help, though they are not a long-term substitute for surgical correction of true valve collapse.
A trial of appropriate medical therapy serves two purposes: it may improve symptoms enough that surgery is not needed, and when it does not, it helps confirm that the remaining problem is structural and therefore likely to respond to surgery. After functional septorhinoplasty, ongoing medical management of allergy or rhinitis is often still part of keeping the nose comfortable.
Specialists who perform functional septorhinoplasty

Dr. Moustafa Mourad
MD, FACS
Double Board-Certified Head & Neck and Facial Plastic & Reconstructive Surgeon
Dr. Moustafa Mourad is a double board-certified head and neck and facial plastic and reconstructive surgeon who cares for the full range of cosmetic and complex conditions affecting the face, head, and neck.
- Facial plastic and reconstructive surgery
- Head and neck cancer surgery
- Microvascular free-flap reconstruction
- Facial trauma and reconstruction
Also caring for this area



Not sure who to see? Our patient coordination team can help match you with the right specialist.
(212) 444-8006Frequently Asked Questions
A septoplasty straightens a deviated septum only. A functional septorhinoplasty addresses the septum and the other structures that control nasal breathing — most importantly the internal and external nasal valves — and can also reshape the external nose when desired. If valve collapse is part of the problem, a septoplasty alone often does not fully relieve the obstruction, which is why a broader functional operation may be recommended.
Only if you want it to. Many functional septorhinoplasties are performed purely to improve breathing with no intended change to appearance. When a patient does want cosmetic refinement — such as reducing a hump or straightening a crooked nose — it is planned together with the breathing work so that the change in shape does not weaken the airway.
Coverage depends on your specific plan and on whether the operation is being done to treat a functional problem such as nasal obstruction. The functional, medically necessary portions of nasal surgery are often considered differently from purely cosmetic changes. Our team can help you understand the documentation involved, but coverage decisions are made by your insurer, not by the practice.
Many surgeons now avoid traditional nasal packing, often using thin soft internal splints instead, which are more comfortable and are usually removed at about a week. Your surgeon will tell you what to expect for your specific operation.
It is normal for the nose to feel more congested at first because of internal swelling. Breathing typically improves over the first several weeks as swelling resolves, and many patients notice a clear improvement within the first few months. Surgery aims to improve the airway but cannot guarantee a perfectly clear nose, particularly if allergy or inflammation is also present.
The nasal valves are the narrowest, most flow-limiting parts of the nasal airway. The internal valve sits partway up the nose where the upper cartilage meets the septum; the external valve is around the nostril rim. Because they are the tightest points, even small amounts of narrowing or collapse here can make the nose feel very blocked. Repairing them — often with cartilage grafts that reinforce the sidewall — is a key part of functional surgery.
Yes. Functional septorhinoplasty principles are central to revision nasal surgery. Revision cases are more complex because of scar tissue and because cartilage may have been removed previously, so additional cartilage from the ear or rib is sometimes needed to rebuild support. A careful evaluation determines what is realistic in your case.
Neither is universally better; they suit different problems. The open approach adds a small, usually well-hidden incision across the columella and gives direct visibility for complex straightening, grafting, and revision work. The closed approach keeps all incisions inside the nostrils and may be appropriate for more limited problems. The right choice depends on your anatomy and goals.
Turbinates are reduced, not removed, when they contribute to obstruction. Preserving turbinate tissue is important because the turbinates warm and humidify the air you breathe; removing too much can cause a dry, uncomfortable nose. Reduction is done in a tissue-preserving way.
It is usually performed under general anesthesia as an outpatient procedure, so most patients go home the same day. The length depends on complexity and commonly ranges from about one to several hours, with revision and complex reconstructive cases taking longer.
Strenuous exercise and heavy lifting are typically restricted for several weeks to protect healing and limit swelling and bleeding. If the nasal bones were repositioned, you may need to keep glasses off the bridge or support them for a period. Your surgeon will give you specific timelines based on your operation.
Surgery aims to improve breathing, and most patients breathe better afterward, but no operation can guarantee the result, and a small number of patients have residual or recurrent obstruction. Properly planned functional surgery specifically reinforces support to reduce the risk of the airway weakening over time, which is one reason functional planning matters even in cosmetic cases.
When inflammation, allergy, or rhinitis may be contributing, treating those first is reasonable and sometimes resolves symptoms without surgery. A trial of appropriate medical therapy also helps confirm that the remaining problem is structural and therefore likely to respond to surgery. If your obstruction is clearly structural — for example, from a significant deviation or valve collapse — your surgeon may discuss proceeding to surgery sooner.
Clinical References
These independent resources from medical and professional organizations offer further reading. They are provided for general education and do not replace a consultation with a clinician.
Related Conditions

1 of 4 · Deviated Septum

Request a consultation about functional septorhinoplasty
Schedule a consultation with our team to discuss whether this procedure is the right option for you.