

Overview
Allergic fungal rhinosinusitis (AFRS) is an intense inflammatory response associated with thick allergic mucin, nasal polyps, and characteristic imaging—not an invasive fungal infection. It is important to separate AFRS from a fungal ball, which is a clump of fungal debris in a single sinus, and from invasive fungal sinusitis, an aggressive infection that mainly affects people with weakened immune systems. Durable care requires both clearing obstructed disease when appropriate and a long-term plan to control inflammation and detect recurrence.
What this evaluation should clarify
A focused evaluation is designed to answer a few key questions:
- What objective evidence distinguishes allergic fungal rhinosinusitis from look-alike conditions?
- Which anatomic, inflammatory, dental, neurologic, infectious, or tumor-related factors may be contributing?
- Which medical, procedural, surgical, or multidisciplinary path best fits the findings and your goals?
Living with allergic fungal rhinosinusitis? The next step is a quiet, unhurried conversation.
Evaluation and treatment pathway
Care generally follows a stepwise path:
- Clarify the symptom pattern, duration, triggers, prior treatment, operations, medications, and relevant medical history.
- Reach a diagnosis by integrating history, nasal endoscopy, CT findings, allergy context, and pathologic examination of mucin or tissue. No single symptom or home mold test establishes AFRS.
- Identify important look-alikes, complications, and contributors before settling on a definitive diagnosis.
- When appropriate, use surgery to remove obstructive allergic mucin and open the sinuses for topical treatment, paired with ongoing anti-inflammatory therapy, allergy management, and endoscopic follow-up, because recurrence is common.
- Set a measurable follow-up plan covering symptom goals, objective reassessment, medication response, and imaging or surveillance when appropriate.
Definition and how it differs from invasive fungal sinusitis
AFRS is a non-invasive, allergic-type inflammatory reaction to environmental fungus. The fungus is not growing into the tissues. By contrast, invasive fungal sinusitis is an aggressive infection that spreads into tissue and usually occurs in people with weakened immune systems, and a fungal ball is a localized collection of fungal material in one sinus. These are managed very differently, which is why an accurate diagnosis matters.
Typical features and imaging pattern
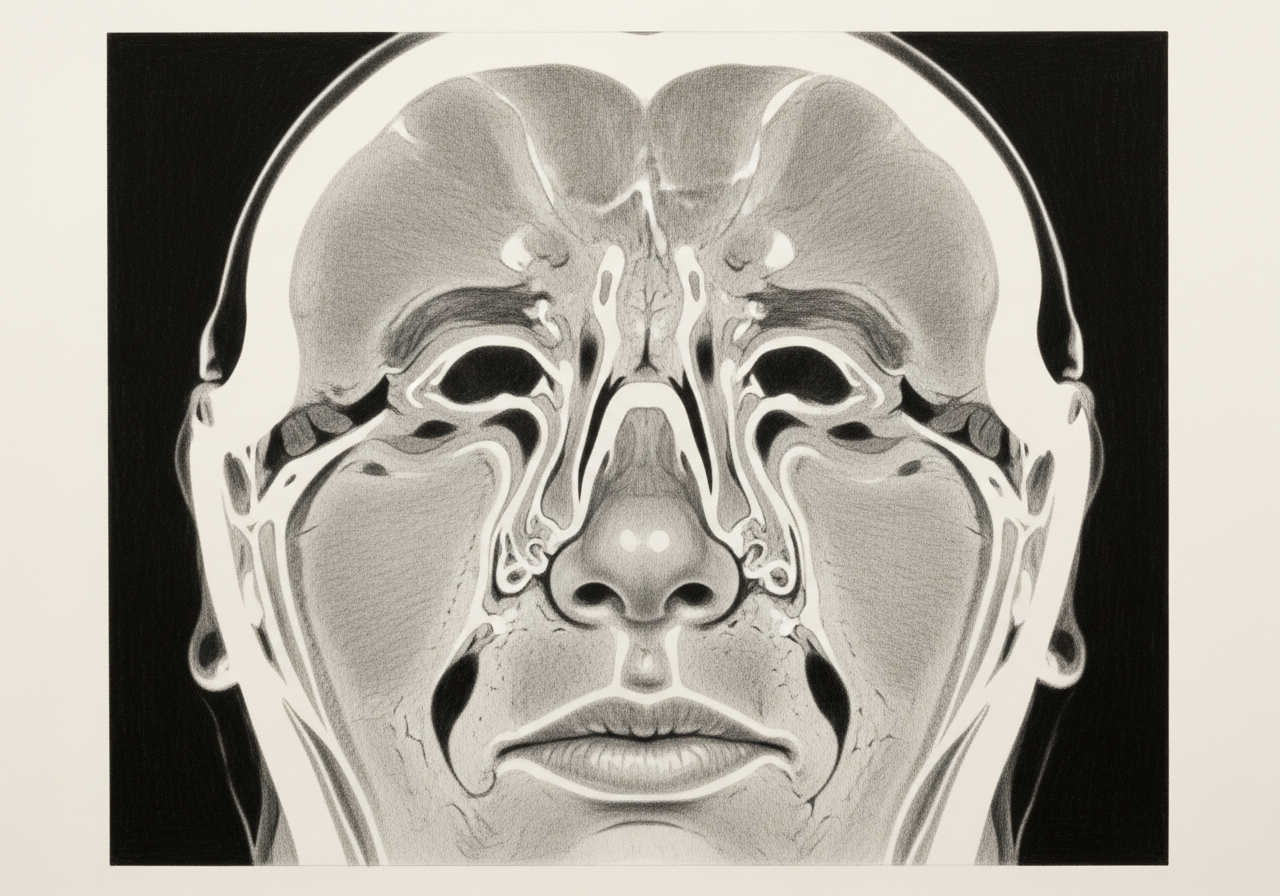
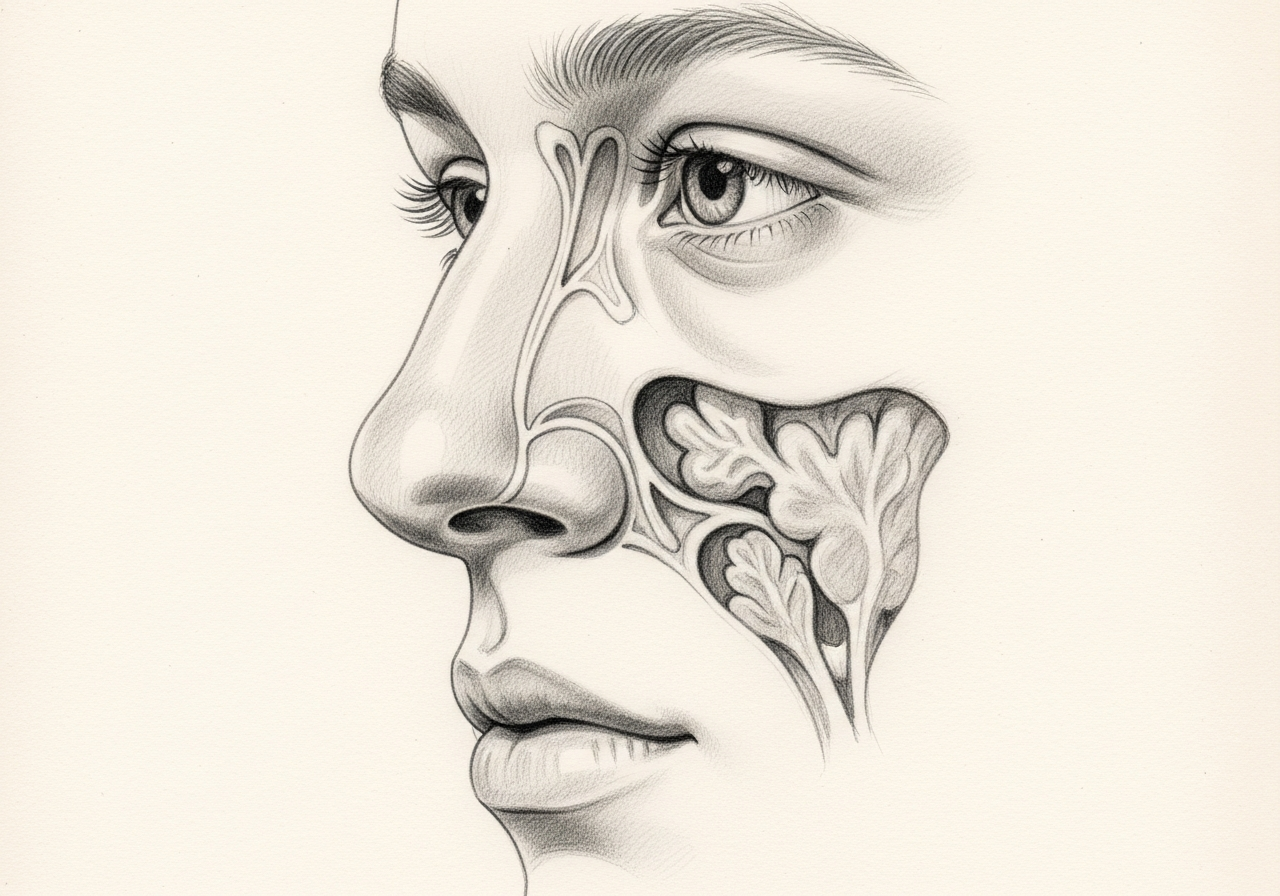
AFRS commonly causes nasal polyps and thick, peanut-butter-like allergic mucin. On CT imaging, affected sinuses often look full with areas of increased density, and the disease can expand the sinus over time. The findings frequently favor one side, although both sides can be involved.
Surgery and medical treatment
Treatment usually combines surgery and medication:
- Endoscopic sinus surgery to remove polyps and allergic mucin and to open the sinuses for topical access
- Topical nasal steroid sprays and steroid rinses afterward
- Saline irrigation to keep the sinuses clear
- Oral corticosteroids in selected situations, under supervision
- Allergy management to reduce the inflammatory drive
Surgery clears disease and creates access for topical medication, but ongoing medical therapy is what helps keep inflammation under control.
Recurrence and surveillance
AFRS can recur because the underlying inflammatory tendency persists. Regular follow-up with endoscopy, continued topical therapy, and prompt attention to returning symptoms help detect and address recurrence early.
What to bring to your consultation
Bringing the right records helps make the visit focused and useful. Where available, gather:
- Imaging files and reports, including CT and any MRI
- Endoscopy or operative findings from prior care
- Pathology results from any biopsy or surgery
- Relevant laboratory results
- Notes from prior treatment and a current medication list
- The specific question you would like answered
When to seek urgent care
Eye swelling, vision change, severe headache, neurologic symptoms, or fever with marked illness or rapid progression needs urgent assessment for a complication or an alternative invasive process.
Medical review
This page is a patient-education resource reviewed by the responsible Norelle Health clinician before publication. It does not replace an in-person evaluation. If symptoms are severe or rapidly worsening, seek immediate medical care.
Specialists who treat allergic fungal rhinosinusitis

Dr. Adrian Ong
MD
Board-Certified Facial Plastic & Reconstructive and Head & Neck Surgeon
Dr. Adrian Ong is a board-certified surgeon who practices exclusively on the face, head, and neck, with expertise spanning rhinoplasty, sinus surgery, facial trauma, reconstruction, and sleep surgery.
- Functional and aesthetic rhinoplasty (including revision)
- Sinus surgery and complex revision sinus surgery
- Facial trauma and nasal fractures
- Head and neck cancer surgery and microvascular reconstruction
Also caring for this area


Not sure who to see? Our patient coordination team can help match you with the right specialist.
(212) 444-8006Frequently Asked Questions
Allergic fungal rhinosinusitis is a noninvasive inflammatory form of chronic rhinosinusitis associated with type I hypersensitivity, nasal polyps, eosinophilic mucin, and characteristic radiographic or operative findings.
Diagnosis integrates history, endoscopy, CT findings, allergy context, and pathologic examination of mucin or tissue. No single symptom or home mold test establishes AFRS.
Surgery is often used to remove obstructive allergic mucin and open the sinuses for topical treatment. Ongoing anti-inflammatory therapy, allergy management, and endoscopic follow-up are important because recurrence is common.
Eye swelling, vision change, severe headache, neurologic symptoms, or fever with marked illness or rapid progression need urgent assessment for a complication or an alternative invasive process.
Clinical References
These independent resources from medical and professional organizations offer further reading. They are provided for general education and do not replace a consultation with a clinician.
Related Procedures

1 of 1 · Endoscopic Sinus Surgery
Related Conditions

Request a consultation for allergic fungal rhinosinusitis
Schedule an evaluation with our team to review your symptoms and the appropriate next steps.