

Overview
Empty nose syndrome is a complex, incompletely understood pattern of paradoxical obstruction, dryness, altered airflow sensation, and distress that may occur after turbinate surgery. These symptoms are real and can significantly affect quality of life, even when the nasal passages look open on examination. Care validates symptoms without overdiagnosing, explains the limits of current testing, and sets realistic expectations for conservative, supportive, and selected reconstructive options. This page is educational and does not replace specialist evaluation.
What this evaluation should clarify
A focused evaluation is designed to answer a few key questions:
- What objective evidence and history support empty nose syndrome rather than another cause of nasal symptoms?
- Which anatomic, inflammatory, neurologic, pulmonary, or psychological factors may be contributing?
- Which conservative, supportive, procedural, or multidisciplinary path best fits the findings and your goals?
Living with empty nose syndrome? The next step is a quiet, unhurried conversation.
Evaluation and treatment pathway
Care generally follows a stepwise path:
- Clarify the symptom pattern, duration, triggers, prior treatment, operations, medications, and relevant medical history.
- There is no single definitive test. Evaluation reviews prior operative records, turbinate anatomy, endoscopy, symptom instruments, airflow perception, response to temporary material testing when appropriate, and alternative nasal, pulmonary, neurologic, or psychological contributors.
- Identify important look-alikes, complications, and contributors before settling on a definitive diagnosis.
- Care may include humidification, saline or emollient strategies, treatment of crusting, sleep and mental-health support, breathing or sensory rehabilitation, and selected reconstructive procedures. Evidence is limited and outcomes vary.
- Set a measurable follow-up plan covering symptom goals, objective reassessment, treatment response, and ongoing support when appropriate.
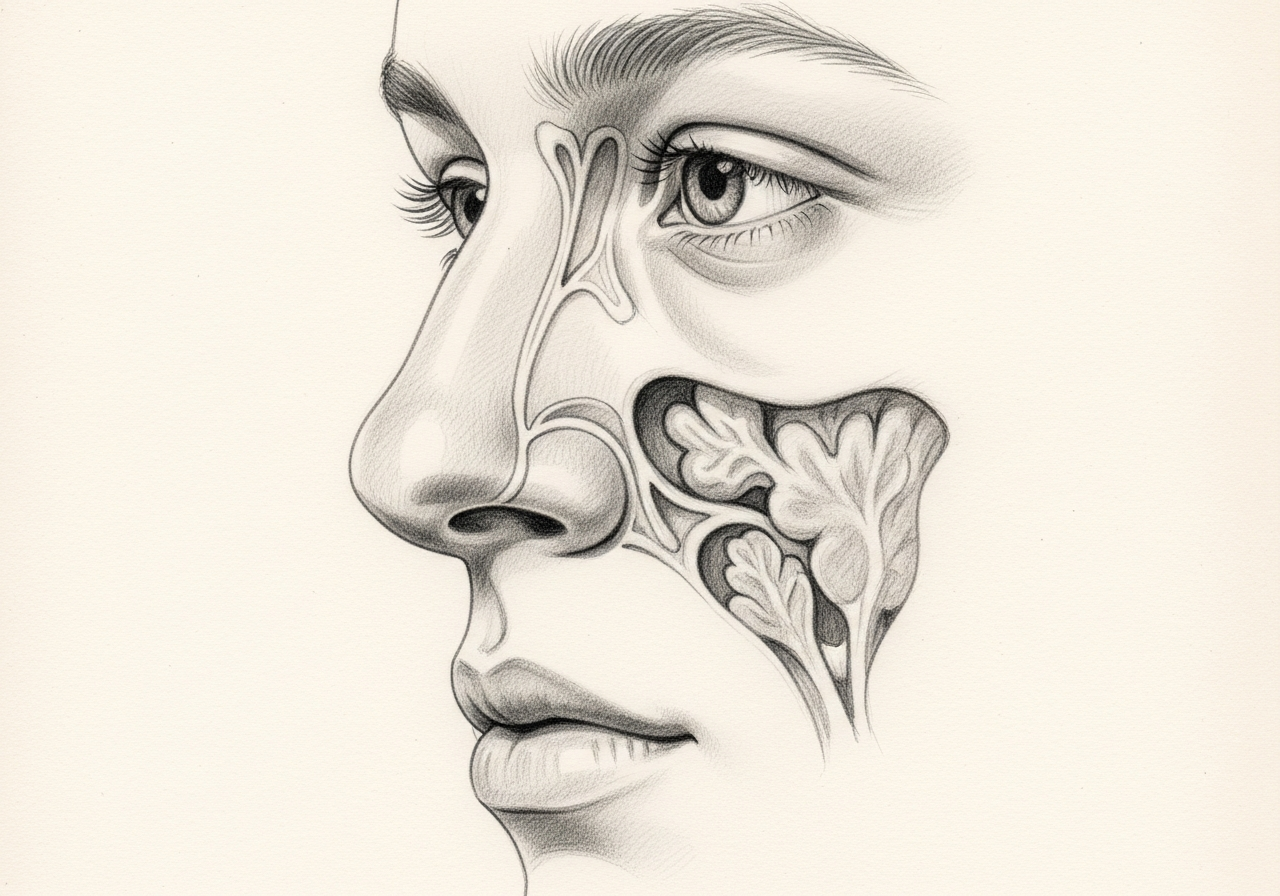
Paradoxical obstruction and dryness
The defining feature of ENS is a feeling of nasal obstruction or insufficient airflow even though the nasal passages appear open. Many people also have ongoing dryness and crusting. The sensation is thought to relate to how the nose senses airflow, not simply to the physical width of the passages.
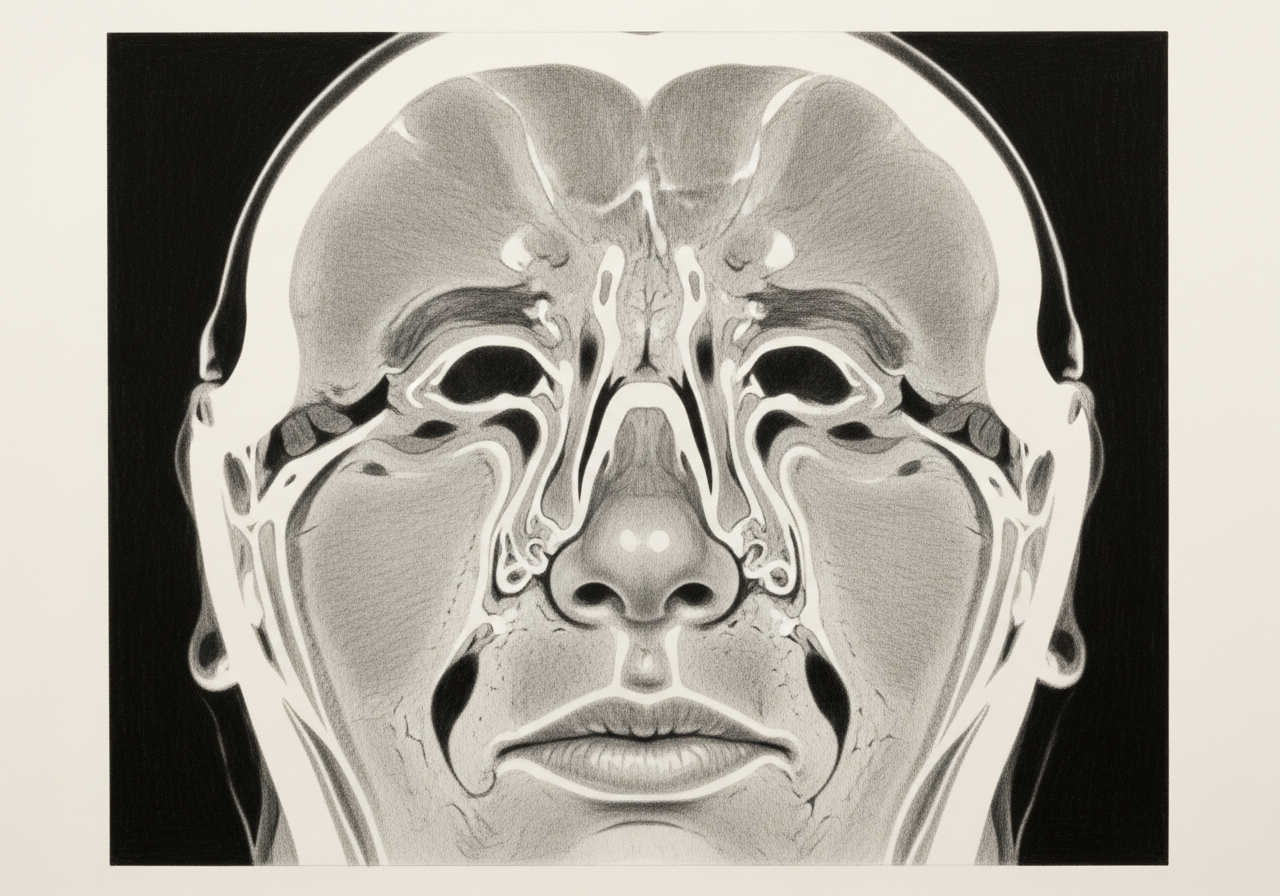
Relationship to prior turbinate surgery without assuming causation
The turbinates help regulate airflow, warming, and humidification, so ENS is sometimes linked to prior turbinate surgery, particularly more aggressive reduction. However, many people have turbinate surgery without developing these symptoms, and the mechanisms are not fully understood, so a previous surgery does not by itself prove the cause.
History, examination, and airflow assessment
Evaluation includes a careful history of the symptoms and any prior nasal surgery, examination with nasal endoscopy, and assessment of airflow. Some clinicians use simple tests, such as temporarily placing material in the nose to see whether it changes the sensation, to help understand the symptoms. The goal is to take the concern seriously and characterize it accurately.
Moisturization and supportive care
First-line care focuses on relieving dryness and improving comfort, using saline sprays, gels, and irrigation, humidification, and measures to address crusting or infection. Many patients gain meaningful relief from consistent supportive care, which is often continued long term.
Selected reconstructive approaches
For some patients whose symptoms persist despite supportive care, reconstructive procedures that add bulk to the nasal sidewall may be considered to alter airflow sensation. These approaches are individualized, are not appropriate or available for everyone, and their results vary, so they are discussed carefully with realistic expectations.
Mental-health support without dismissing physical symptoms
ENS symptoms can be very distressing and may affect sleep, concentration, and mood. Acknowledging this distress and offering support for overall well-being is an important part of care, alongside, and never instead of, taking the physical symptoms seriously.
What to bring to your consultation
Bringing the right records helps make the visit focused and useful. Where available, gather:
- Imaging files and reports, including CT and any MRI
- Endoscopy or operative findings from prior care
- Pathology results from any biopsy or surgery
- Relevant laboratory results
- Notes from prior treatment and a current medication list
- The specific question you would like answered
When to seek urgent care
Severe breathing distress needs urgent medical assessment even when the anatomy appears open. Thoughts of self-harm, an inability to stay safe, or an overwhelming psychological crisis require immediate emergency or crisis support.
Medical review
This page is a patient-education resource reviewed by the responsible Norelle Health clinician before publication. It does not replace an in-person evaluation. If symptoms are severe or rapidly worsening, seek immediate medical care.
Specialists who treat empty nose syndrome

Dr. Adrian Ong
MD
Board-Certified Facial Plastic & Reconstructive and Head & Neck Surgeon
Dr. Adrian Ong is a board-certified surgeon who practices exclusively on the face, head, and neck, with expertise spanning rhinoplasty, sinus surgery, facial trauma, reconstruction, and sleep surgery.
- Functional and aesthetic rhinoplasty (including revision)
- Sinus surgery and complex revision sinus surgery
- Facial trauma and nasal fractures
- Head and neck cancer surgery and microvascular reconstruction
Also caring for this area


Not sure who to see? Our patient coordination team can help match you with the right specialist.
(212) 444-8006Frequently Asked Questions
In empty nose syndrome, the sensation of obstruction relates to how the nose senses airflow rather than the physical width of the passages. The passages can look open while breathing still feels abnormal, and these symptoms are real.
There is no single definitive test. Evaluation reviews prior operative records, turbinate anatomy, endoscopy, symptom instruments, airflow perception, response to temporary material testing when appropriate, and alternative nasal, pulmonary, neurologic, or psychological contributors.
No. Care may include humidification, saline or emollient strategies, treatment of crusting, sleep and mental-health support, and breathing or sensory rehabilitation, with selected reconstructive procedures considered for some patients. Evidence is limited and outcomes vary.
Severe breathing distress needs urgent medical assessment even when the anatomy appears open. Thoughts of self-harm, an inability to stay safe, or an overwhelming psychological crisis require immediate emergency or crisis support.
Clinical References
These independent resources from medical and professional organizations offer further reading. They are provided for general education and do not replace a consultation with a clinician.
Related Procedures

1 of 2 · Nasal Valve Repair
Related Conditions

Request a consultation for empty nose syndrome
Schedule an evaluation with our team to review your symptoms and the appropriate next steps.