

Overview
Facial pressure, congestion, and watery eyes can occur during migraine, so the location of pain does not prove a sinus infection. Many headaches labeled as sinus headaches are in fact migraine, and the treatments are very different. Evaluation focuses on which nasal findings support rhinosinusitis, which headache features point toward migraine, and why a normal endoscopy or CT can redirect care rather than end the evaluation. This page is educational and does not diagnose the cause of any individual's headache.
What this evaluation should clarify
A focused evaluation is designed to answer a few key questions:
- What objective evidence distinguishes true sinus disease from migraine and other headache disorders?
- Which anatomic, inflammatory, dental, neurologic, infectious, or tumor-related factors may be contributing?
- Which medical, procedural, or multidisciplinary path best fits the findings and your goals?
Living with sinus headache versus migraine? The next step is a quiet, unhurried conversation.
Evaluation and treatment pathway
Care generally follows a stepwise path:
- Clarify the symptom pattern, duration, triggers, prior treatment, operations, medications, and relevant medical history.
- Evaluation combines headache pattern, nausea, light or sound sensitivity, activity effects, duration, and triggers with nasal symptoms, endoscopy, and selective imaging. Objective sinus findings must match the symptom pattern.
- Identify important look-alikes, complications, and contributors before settling on a definitive diagnosis.
- Treatment follows the diagnosis: guideline-based sinus care for objective rhinosinusitis, migraine-directed care or neurology referral when features support a primary headache disorder, and evaluation for dental, neuralgic, or other facial pain causes when appropriate.
- Set a measurable follow-up plan covering symptom goals, objective reassessment, medication response, and imaging or surveillance when appropriate.
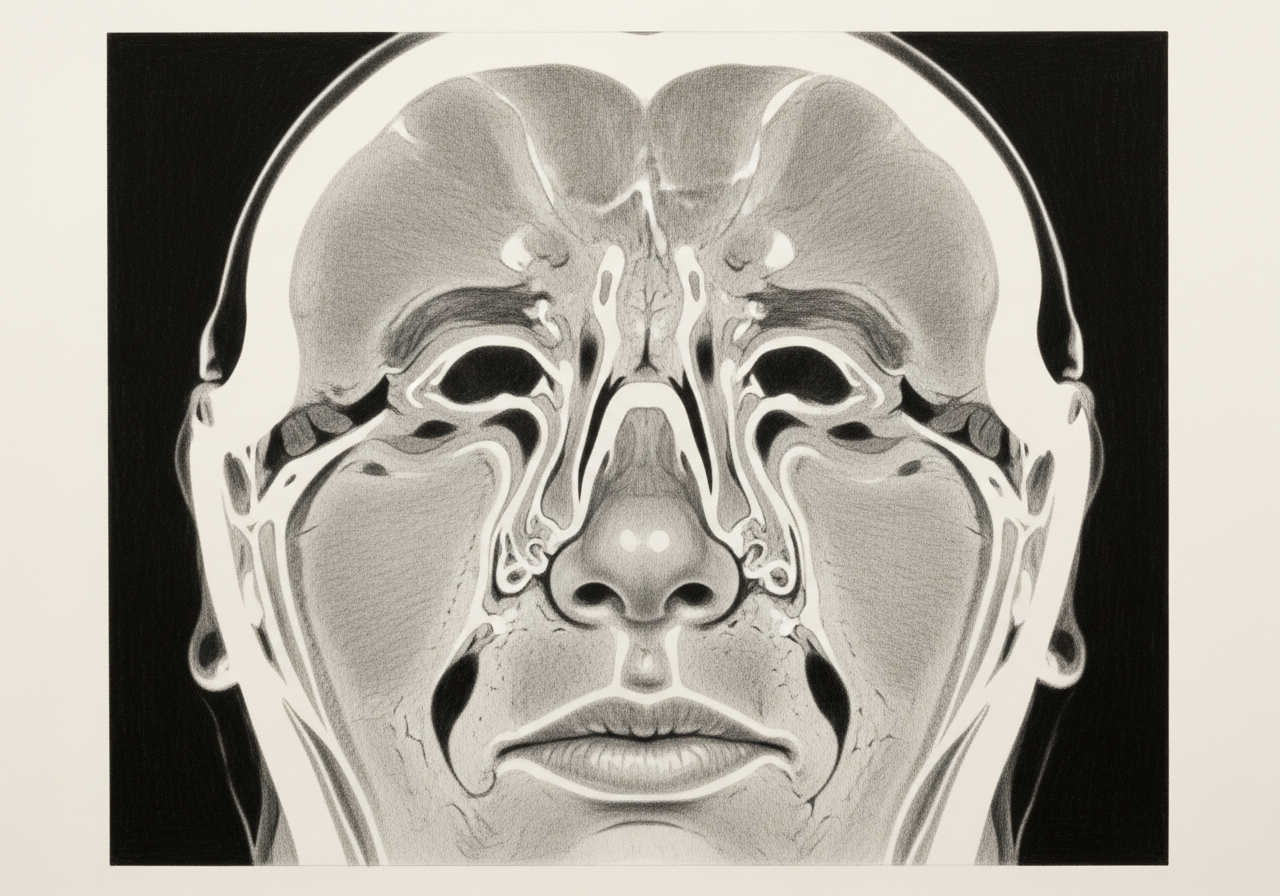
Why pressure and congestion can overlap with migraine
Migraine activates nerve pathways in the face and head that can produce facial pressure, pain, and even nasal congestion or a runny nose during attacks. Because these features resemble sinusitis, many headaches are mistakenly attributed to the sinuses. Recognizing this overlap is the first step to an accurate diagnosis.
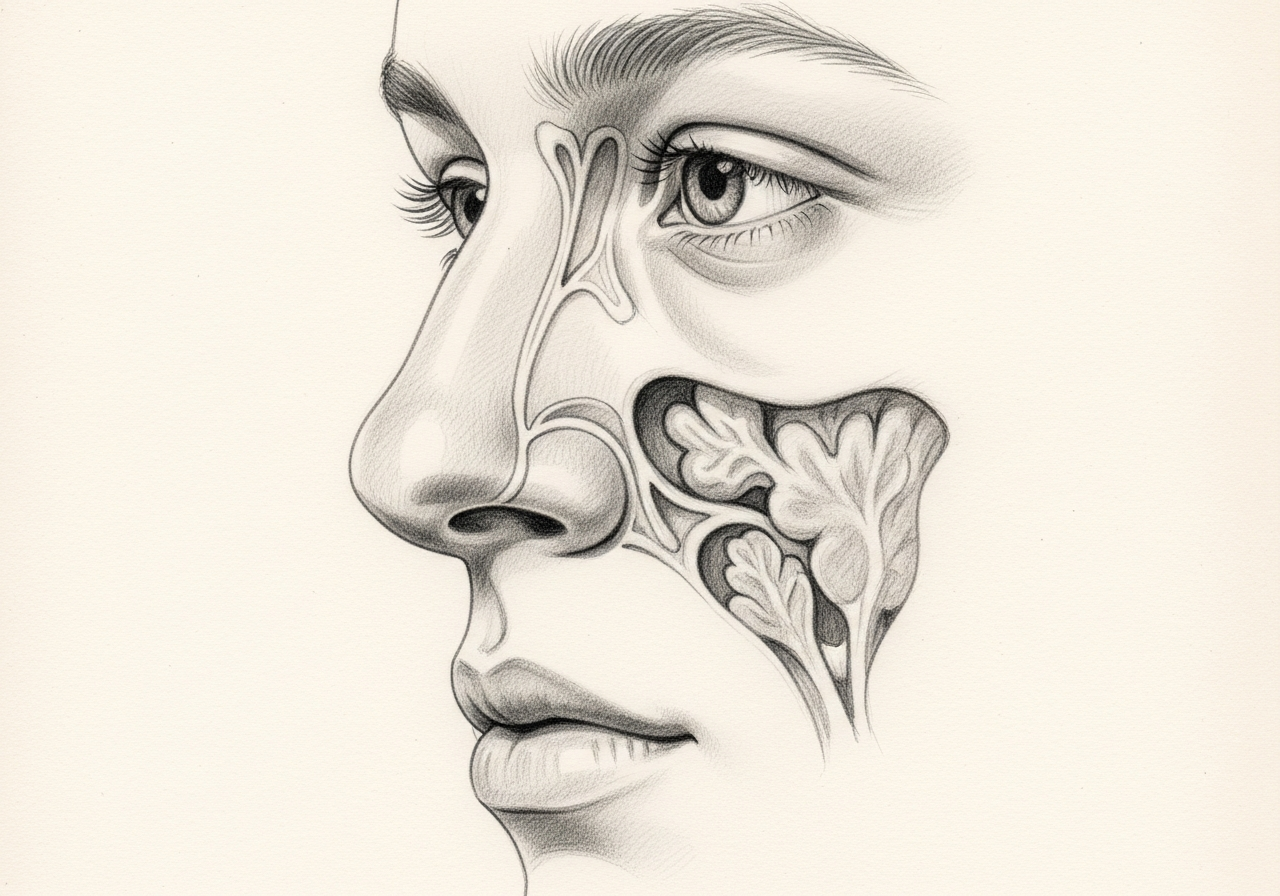
Symptoms that support objective sinus disease
True sinus disease is more likely when there are objective findings such as discolored nasal drainage, fever, or signs of infection on examination, and when nasal endoscopy or imaging shows inflammation. Features such as throbbing one-sided headache, sensitivity to light or sound, nausea, or a pattern of recurrent disabling episodes point more toward migraine.
Nasal endoscopy and imaging limitations
Nasal endoscopy lets a clinician look directly for inflammation or drainage, and CT imaging can show sinus disease. However, a normal CT does not rule out every cause of facial pain, and incidental minor findings on imaging do not prove that the sinuses are the source of a headache. Results are interpreted together with the history.
When neurology evaluation is helpful
When the pattern suggests migraine or another primary headache disorder, evaluation and treatment with neurology are often the most helpful next step. Coordinating between rhinology and neurology helps ensure that both sinus and headache causes are properly considered.
Avoiding unnecessary antibiotics or surgery
Misattributing migraine to the sinuses can lead to repeated antibiotic courses or even sinus surgery that does not relieve the headache. Sinus surgery is directed at objective sinus disease, not at headache alone, so an accurate diagnosis protects patients from treatments unlikely to help.
What to bring to your consultation
Bringing the right records helps make the visit focused and useful. Where available, gather:
- Imaging files and reports, including CT and any MRI
- Endoscopy or operative findings from prior care
- Pathology results from any biopsy or surgery
- Relevant laboratory results
- Notes from prior treatment and a current medication list
- The specific question you would like answered
When to seek urgent care
A sudden "worst headache," a new neurologic deficit, confusion, fainting, fever with neck stiffness, acute vision change, severe headache after trauma, or a new high-risk headache pattern requires emergency evaluation.
Medical review
This page is a patient-education resource reviewed by the responsible Norelle Health clinician before publication. It does not replace an in-person evaluation. If symptoms are severe or rapidly worsening, seek immediate medical care.
Specialists who treat sinus headache versus migraine

Dr. Adrian Ong
MD
Board-Certified Facial Plastic & Reconstructive and Head & Neck Surgeon
Dr. Adrian Ong is a board-certified surgeon who practices exclusively on the face, head, and neck, with expertise spanning rhinoplasty, sinus surgery, facial trauma, reconstruction, and sleep surgery.
- Functional and aesthetic rhinoplasty (including revision)
- Sinus surgery and complex revision sinus surgery
- Facial trauma and nasal fractures
- Head and neck cancer surgery and microvascular reconstruction
Also caring for this area


Not sure who to see? Our patient coordination team can help match you with the right specialist.
(212) 444-8006Frequently Asked Questions
Yes. Migraine can cause facial pressure, congestion, and even a runny nose during attacks, which is one reason migraine is often mistaken for a sinus headache. The location of pain does not prove a sinus infection.
Evaluation combines headache pattern, nausea, light or sound sensitivity, activity effects, duration, and triggers with nasal symptoms, endoscopy, and selective imaging. Objective sinus findings must match the symptom pattern.
No. Treatment follows the diagnosis: guideline-based sinus care for objective rhinosinusitis, migraine-directed care or neurology referral when features support a primary headache disorder, and evaluation for dental, neuralgic, or other facial pain causes when appropriate.
A sudden "worst headache," a new neurologic deficit, confusion, fainting, fever with neck stiffness, acute vision change, severe headache after trauma, or a new high-risk headache pattern requires emergency evaluation.
Clinical References
These independent resources from medical and professional organizations offer further reading. They are provided for general education and do not replace a consultation with a clinician.
Related Conditions

1 of 4 · Chronic Sinusitis
Request a consultation for sinus headache versus migraine
Schedule an evaluation with our team to review your symptoms and the appropriate next steps.