

Overview
Skull base osteomyelitis is a potentially serious infection of the bone at the base of the skull. It often requires hospital-level evaluation, prolonged antimicrobial treatment, and coordinated care across ENT, infectious disease, radiology, and, in selected cases, surgery.
Recognizing it early matters, because it is not a routine outpatient sinus infection. Deep, persistent pain and new cranial-nerve symptoms, particularly in people with diabetes or a weakened immune system, are important warning signs that the infection may be spreading into the skull base.
What this evaluation should clarify
A focused evaluation is meant to answer a few key questions:
- What objective evidence distinguishes skull base osteomyelitis from conditions that can look similar?
- Which contributors, such as a severe ear or sinus infection, diabetes, immune compromise, or a tumor that can mimic infection, need to be considered?
- Which medical, procedural, surgical, or multidisciplinary path best fits the findings and your goals?
Evaluation and treatment pathway
Care usually follows a stepwise pathway:
- Review the symptom pattern, duration, triggers, prior treatment, operations, medications, and relevant medical history.
- Combine risk factors such as diabetes or immune compromise with the ear or nasal examination, inflammatory markers, CT and MRI, nuclear imaging in selected cases, and cultures or tissue sampling when needed.
- Identify important look-alikes, complications, and contributors before settling on a diagnosis.
- Treatment commonly involves prolonged targeted antimicrobial therapy, control of contributing conditions, repeated clinical and imaging assessment, and selective surgery for diagnosis, drainage, or source control rather than routine bone removal.
- Set a clear follow-up plan, including symptom goals, objective reassessment, medication response, and imaging or surveillance when appropriate.
Risk factors and cranial-nerve symptoms
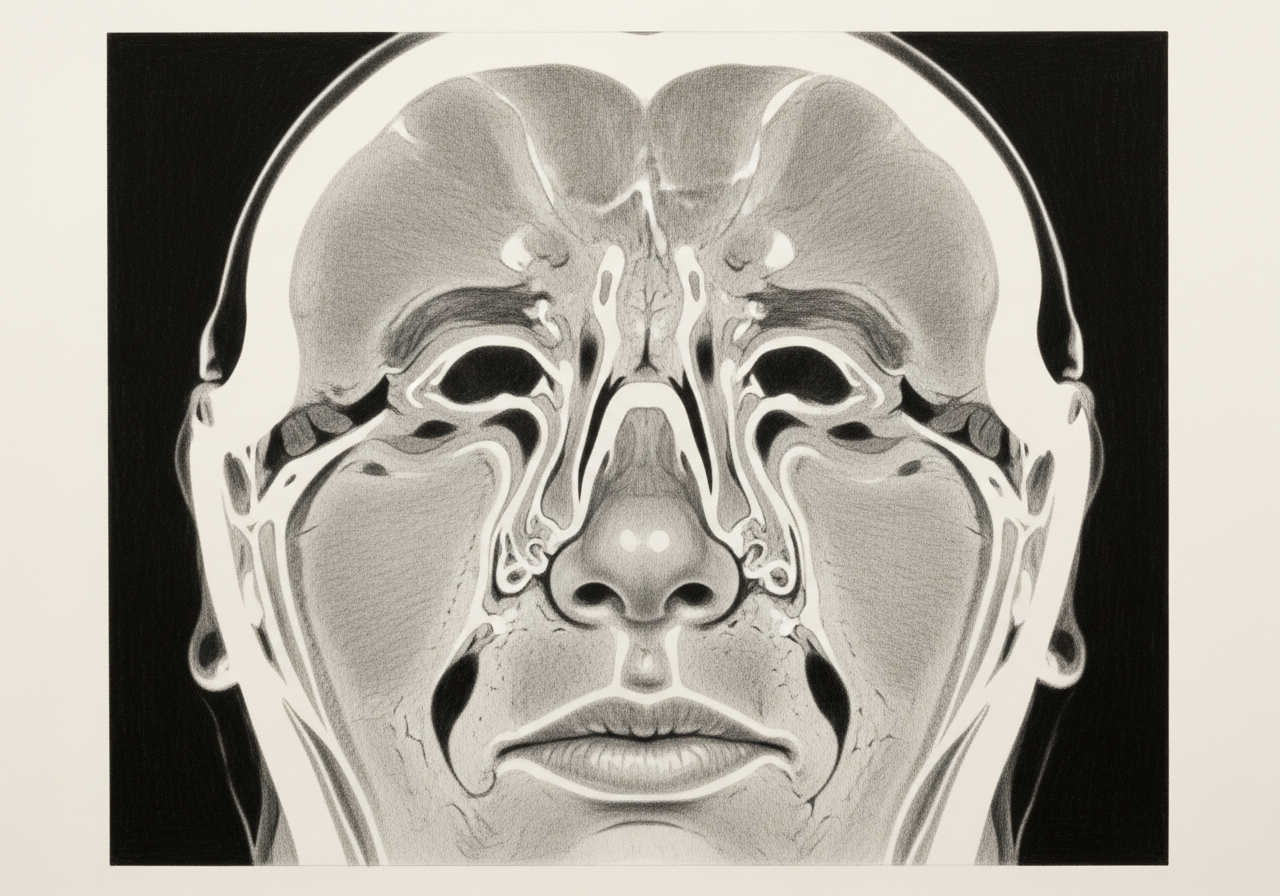
It most often affects people with diabetes or a weakened immune system. Because numerous cranial nerves pass through the skull base, the infection can cause facial weakness, difficulty swallowing, hoarseness, or hearing changes, along with deep, persistent headache. New cranial-nerve symptoms in this setting are an important warning sign.
Imaging, culture, and biopsy
Diagnosis combines imaging, such as CT and MRI and sometimes nuclear medicine studies, with cultures to identify the responsible organism. A biopsy may be needed both to confirm infection and to rule out a tumor that can mimic it. Identifying the organism guides targeted treatment.
Hospital-based antimicrobial treatment
Treatment centers on a prolonged course of targeted antimicrobial therapy, often given intravenously and coordinated with infectious disease specialists. Controlling diabetes and other contributing conditions is an important part of care. This is hospital-based treatment rather than a brief outpatient course.
Role of surgery or debridement
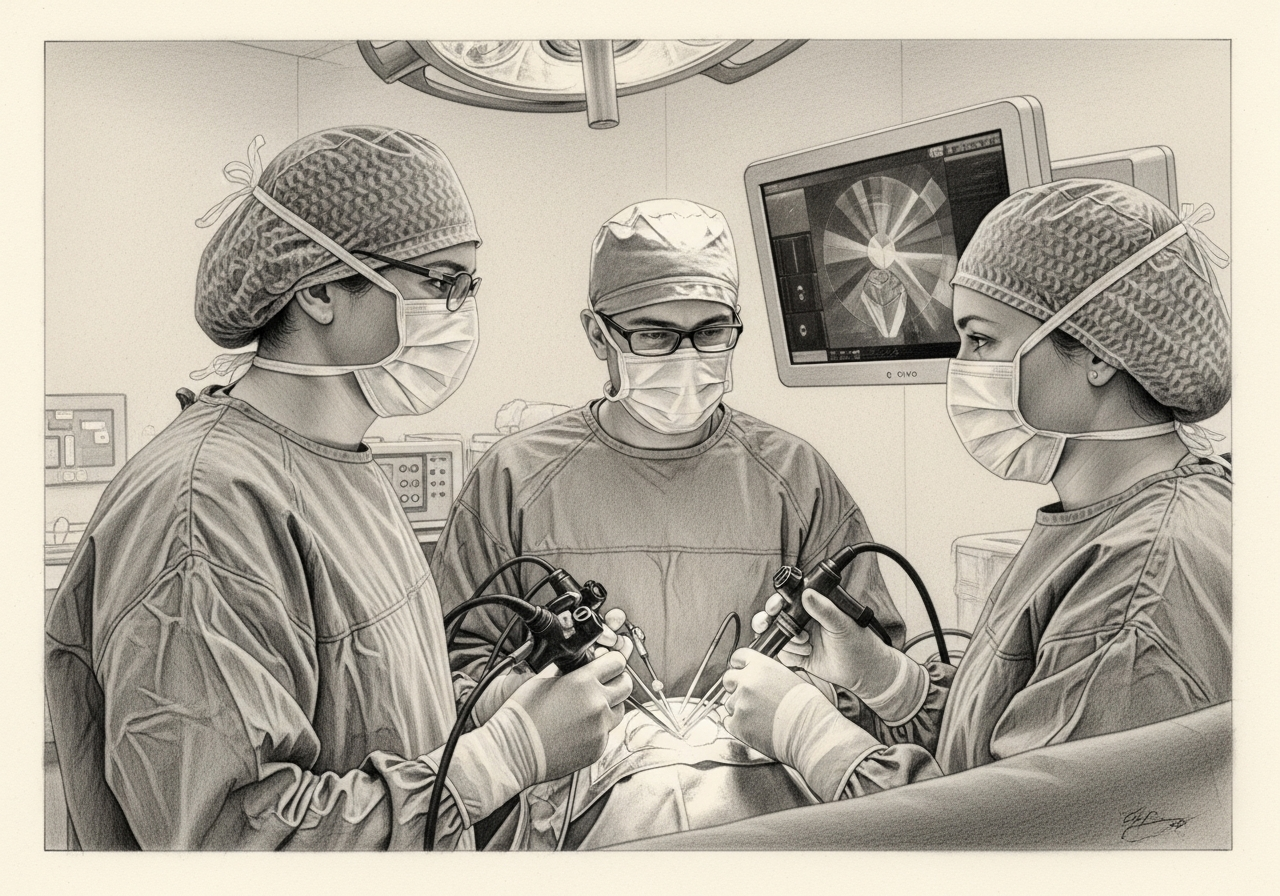
Surgery is not always required, but debridement of infected or dead tissue, drainage, or obtaining tissue for diagnosis may be needed in selected cases. The decision depends on the extent of disease and the response to medical treatment.
Long-term monitoring
Because the infection involves bone and can recur, treatment is often lengthy and followed by ongoing clinical and imaging monitoring to confirm the infection is controlled. Care is coordinated across multiple specialties.
What to bring to your consultation
To make the most of your visit, bring or securely share the records that can change the plan:
- Imaging files and reports, such as CT or MRI
- Endoscopy or operative findings
- Pathology results
- Laboratory results
- Notes from prior treatment
- A current medication list
- The specific question you would like answered
When to seek urgent care
Severe, unrelenting ear or deep facial pain, new facial weakness, double vision, a change in swallowing or voice, confusion, fever, severe headache, or other cranial-nerve symptoms calls for urgent hospital assessment, especially with diabetes or a weakened immune system. An online form or routine appointment request is not an emergency service; for these symptoms, seek immediate in-person care.
Medical review
This page is a patient-education resource reviewed by the responsible Norelle Health clinician before publication. It does not replace an in-person evaluation. If symptoms are severe or rapidly worsening, seek immediate medical care.
Specialists who treat skull base osteomyelitis

Dr. Adrian Ong
MD
Board-Certified Facial Plastic & Reconstructive and Head & Neck Surgeon
Dr. Adrian Ong is a board-certified surgeon who practices exclusively on the face, head, and neck, with expertise spanning rhinoplasty, sinus surgery, facial trauma, reconstruction, and sleep surgery.
- Functional and aesthetic rhinoplasty (including revision)
- Sinus surgery and complex revision sinus surgery
- Facial trauma and nasal fractures
- Head and neck cancer surgery and microvascular reconstruction
Also caring for this area


Not sure who to see? Our patient coordination team can help match you with the right specialist.
(212) 444-8006Frequently Asked Questions
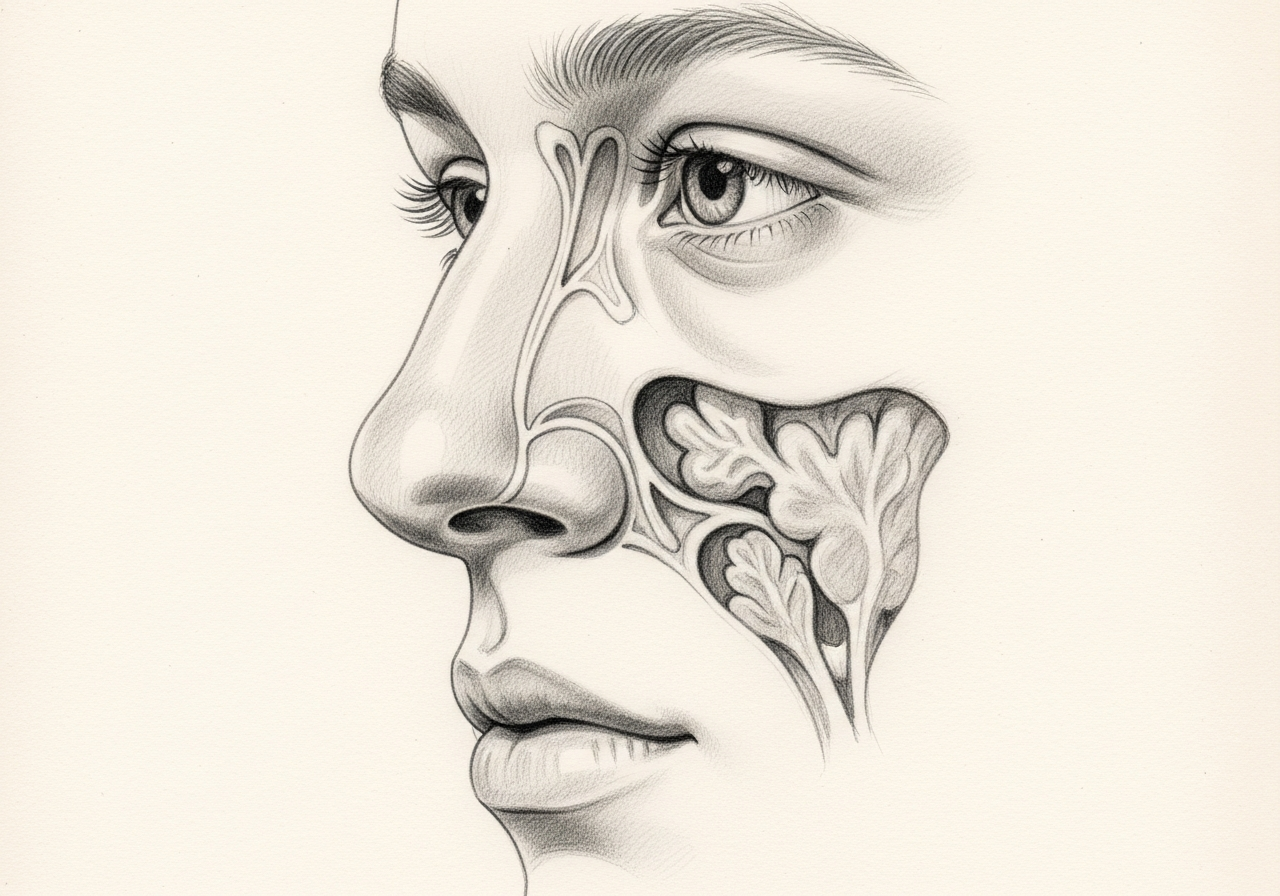
Skull base osteomyelitis is infection and inflammation of the bone at the base of the skull. It classically arises from a severe external-ear infection but can also occur centrally or spread from the sinonasal area and other sources.
Diagnosis combines risk factors such as diabetes or immune compromise with severe persistent pain, cranial-nerve findings, an ear or nasal examination, inflammatory markers, CT and MRI, nuclear imaging in selected cases, and microbiologic or tissue sampling when needed.
No. Treatment commonly involves prolonged targeted antimicrobial therapy, control of contributing disease, and repeated clinical and imaging assessment. Surgery is used selectively for diagnosis, drainage, or source control rather than routine bone removal.
Severe, unrelenting ear or deep facial pain, new facial weakness, double vision, a change in swallowing or voice, confusion, fever, severe headache, or other cranial-nerve symptoms calls for urgent hospital assessment, especially with diabetes or immune compromise.
Clinical References
These independent resources from medical and professional organizations offer further reading. They are provided for general education and do not replace a consultation with a clinician.
Related Procedures

1 of 1 · Endoscopic Skull Base Surgery
Related Conditions

1 of 2 · Sphenoid Sinus Disease
Request a consultation for skull base osteomyelitis
Schedule an evaluation with our team to review your symptoms and the appropriate next steps.