

About the Procedure
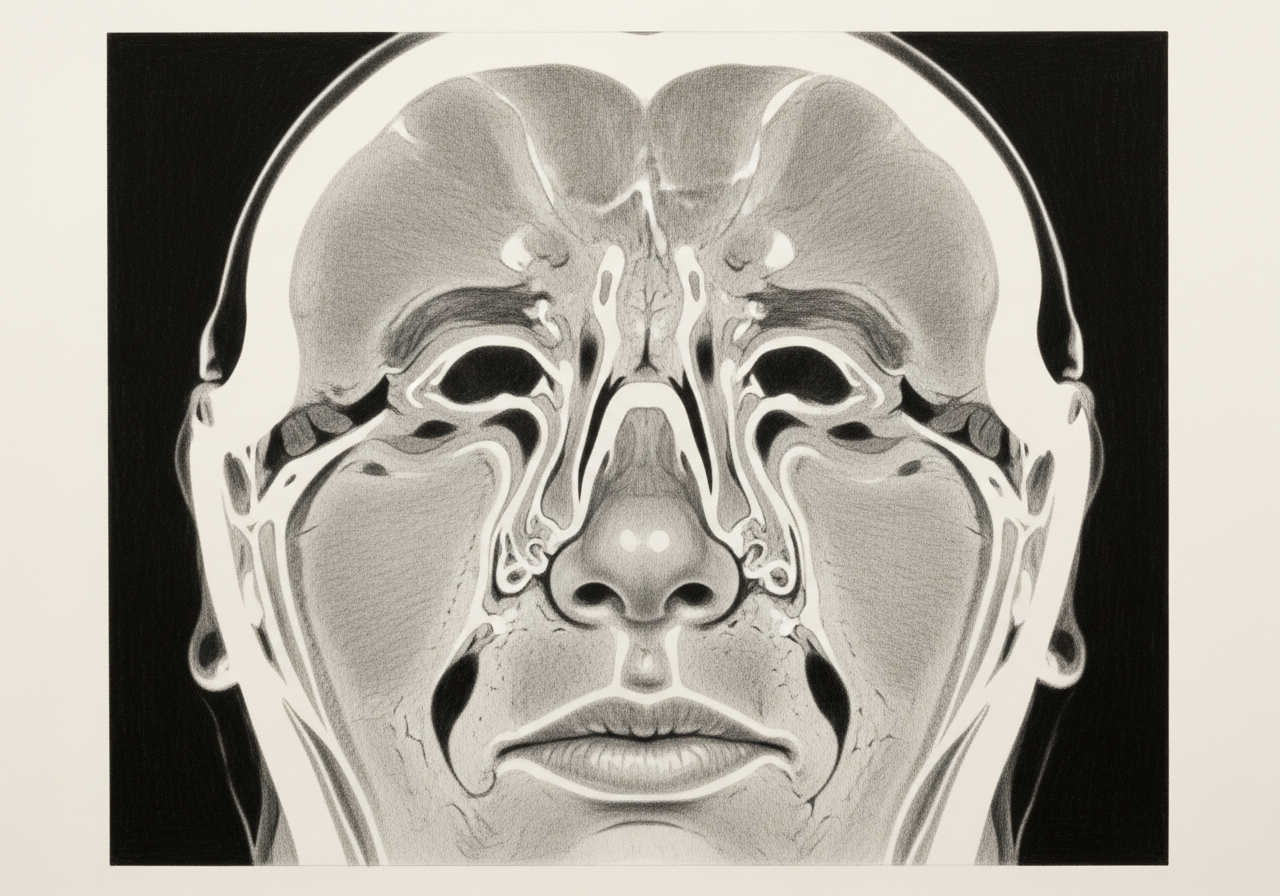
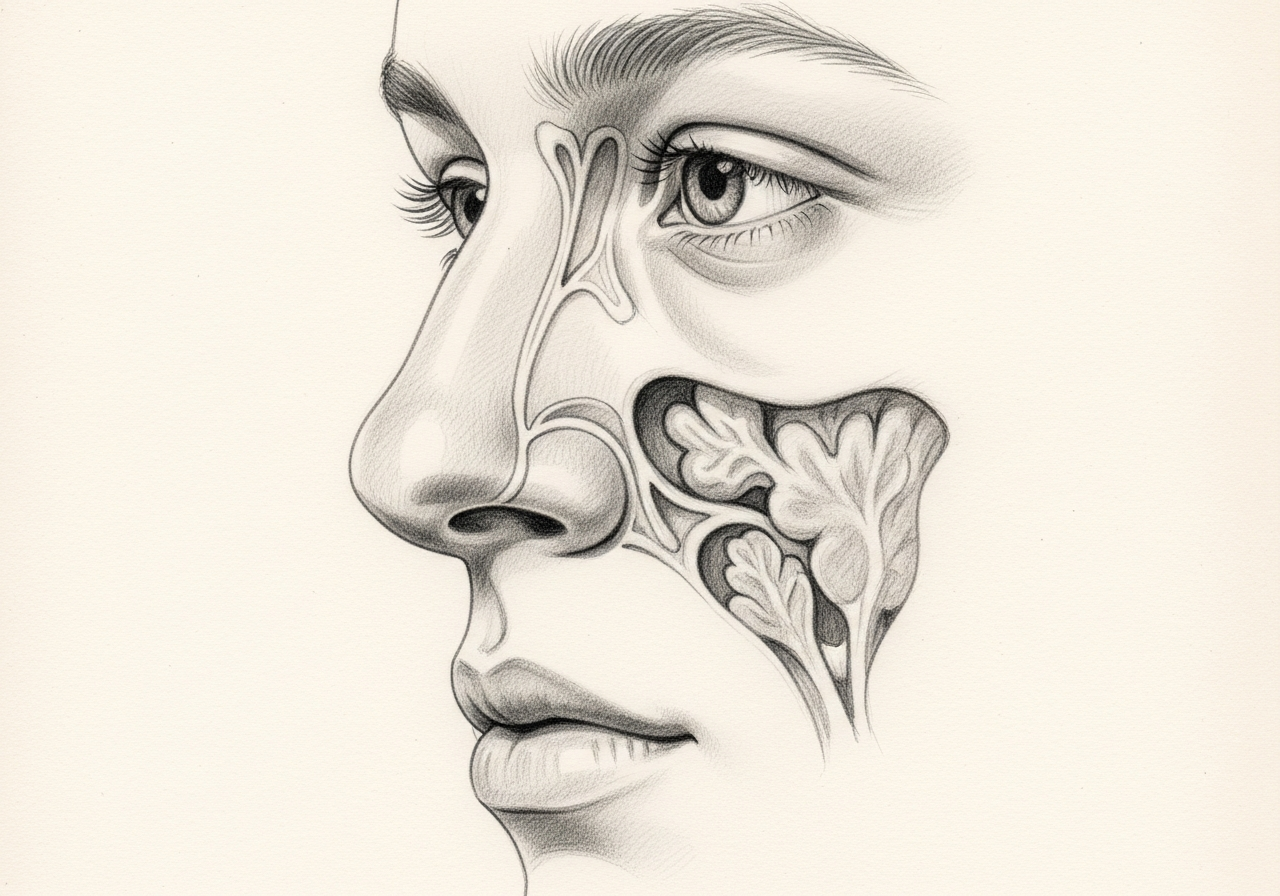
The eye socket (orbit) shares thin bony walls with the nose and sinuses. An endoscopic endonasal route can reach selected lesions of the inner (medial) or lower (inferior) orbit through the nose, without an external incision.
Not every orbital problem can be treated this way. Candidacy depends on the precise location of the problem, its pathology, vision and eye-movement status, how vascular the lesion is, and whether an external or combined approach would offer safer access. Lesions on the outer side of the orbit or wrapped around the eye often need an external or combined approach, and some are better managed without surgery.
At Norelle Health, endoscopic orbital surgery is performed in close partnership with ophthalmology and, when the skull base is involved, neurosurgery. Careful evaluation determines whether an endonasal route is appropriate and what the realistic goals and risks are.
What this evaluation should clarify
This page is meant to help you understand a few key decisions before considering endoscopic orbital surgery:
- Whether the diagnosis and treatment goal are established with the right examination, imaging, and any biopsy
- How an endonasal approach compares with observation, medication, an external or combined approach, decompression, or oncologic treatment
- Which factors — the location and pathology of the problem, your vision and eye-movement status, and the balance of benefits and risks — change the recommendation
Considering endoscopic orbital surgery? The next step is a quiet, unhurried conversation.
Evaluation and treatment pathway
- Confirm the diagnosis, the goal of treatment, and the reasons a less invasive or nonsurgical approach is not enough.
- Candidacy requires detailed CT or MRI localization, an ophthalmic examination, a clear differential diagnosis, and a plan for tissue, vascular, or infectious risks. Not every orbital lesion can be reached or is appropriately treated through the nose.
- Alternatives include observation, medication, image-guided biopsy, external orbitotomy, combined surgery, decompression, or oncologic therapy, depending on the pathology and the part of the orbit involved.
- The surgeon opens a corridor through the nose and sinuses and reaches the selected orbital wall or lesion while protecting the eye muscles, optic nerve, tear-drainage structures, and blood vessels. Ophthalmic participation depends on the case and is made explicit.
- Postoperative care monitors vision, pupils, eye movement, double vision, bleeding, swelling, and nasal healing. Because some orbital complications are time-sensitive, the emergency plan is immediate.
Conditions that may use an endonasal orbital route
An endoscopic endonasal route may be used in selected cases for:
- Decompression of the orbit, most often for thyroid eye disease
- Drainage of an orbital or subperiosteal abscess related to sinus infection
- Biopsy of an orbital lesion to establish a diagnosis
- Removal of certain tumors along the medial wall or orbital apex
Whether this route is suitable depends on the exact location of the problem and its relationship to the eye, the optic nerve, and the sinuses.
Roles of ENT and ophthalmology
Endoscopic orbital surgery is a shared effort. The ENT (rhinology) surgeon provides safe endonasal access through the nose and sinuses and works along the orbital wall, while ophthalmology evaluates and manages the eye itself and its function.
When the problem extends to the skull base, neurosurgery is also involved. This team approach helps protect vision and address the underlying condition together rather than in isolation.
Endoscopic, external and combined approaches
The endonasal endoscopic route avoids an external incision and is well suited to the inner wall, floor, and back of the orbit. An external approach, through the eyelid or skin, may be needed for the outer orbit or areas the endoscope cannot reach. Some operations combine both routes.
The approach is selected to match the location of the problem while protecting the optic nerve, the eye muscles, and surrounding structures. The plan, including its limits, is discussed before surgery.
Visual-risk counseling and follow-up
Because surgery is performed close to the eye and optic nerve, there are uncommon but serious risks to vision and eye movement, including double vision. These risks, and the realistic goals of the operation, are reviewed in detail beforehand.
After surgery, vision, eye position, and movement are monitored closely, and nasal healing is supported with saline rinses and follow-up endoscopy. Care is coordinated between the surgical team and ophthalmology.
What to bring to your consultation
Bringing the right records helps make the most of your visit. Where possible, bring or securely transfer:
- Imaging files and reports (such as CT or MRI of the orbit and sinuses)
- Any prior endoscopy or operative findings
- Pathology results, if a biopsy has been done
- Relevant laboratory results
- Notes from prior treatment and a current medication list
- The specific question you would most like answered
For complex orbital or tumor care, your records may be reviewed with the specialists involved in that part of your evaluation.
When to seek urgent care
Some symptoms need emergency assessment rather than a routine appointment. Seek immediate care for sudden vision loss, severe eye pain, rapidly increasing swelling, new marked double vision, a change in the pupil, heavy bleeding, a severe headache, or any neurologic symptom after surgery.
These can indicate an infection spreading into the orbit, pressure on the optic nerve, or another time-sensitive process. An online form or routine appointment request is not an emergency service.
Medical review
This page is a patient-education resource reviewed by the responsible Norelle Health clinician before publication. It does not replace an in-person evaluation. Sudden vision loss, a rapidly bulging or very painful eye, double vision, or eye redness and swelling with fever should be treated as an emergency, and you should seek immediate medical care.
Specialists who perform endoscopic orbital surgery

Dr. Adrian Ong
MD
Board-Certified Facial Plastic & Reconstructive and Head & Neck Surgeon
Dr. Adrian Ong is a board-certified surgeon who practices exclusively on the face, head, and neck, with expertise spanning rhinoplasty, sinus surgery, facial trauma, reconstruction, and sleep surgery.
- Functional and aesthetic rhinoplasty (including revision)
- Sinus surgery and complex revision sinus surgery
- Facial trauma and nasal fractures
- Head and neck cancer surgery and microvascular reconstruction
Also caring for this area


Not sure who to see? Our patient coordination team can help match you with the right specialist.
(212) 444-8006Frequently Asked Questions
Candidacy requires detailed CT or MRI localization, an ophthalmic examination, a clear differential diagnosis, and a plan for tissue, vascular, or infectious risks. Not every orbital lesion can be reached or is appropriately treated through the nose.
The surgeon opens a corridor through the nose and sinuses and reaches the selected orbital wall or lesion while protecting the eye muscles, optic nerve, tear-drainage structures, and blood vessels. Ophthalmic participation depends on the case and is made explicit.
Alternatives include observation, medication, image-guided biopsy, external orbitotomy, combined surgery, decompression, or oncologic therapy, depending on the pathology and the part of the orbit involved.
Postoperative care monitors vision, pupils, eye movement, double vision, bleeding, swelling, and nasal healing. Because some orbital complications are time-sensitive, the emergency plan is immediate.
Clinical References
These independent resources from medical and professional organizations offer further reading. They are provided for general education and do not replace a consultation with a clinician.
Related Conditions

Related Procedures

1 of 3 · Orbital Decompression
Request a consultation about endoscopic orbital surgery
Schedule a consultation with our team to discuss whether this procedure is the right option for you.