

About the Procedure
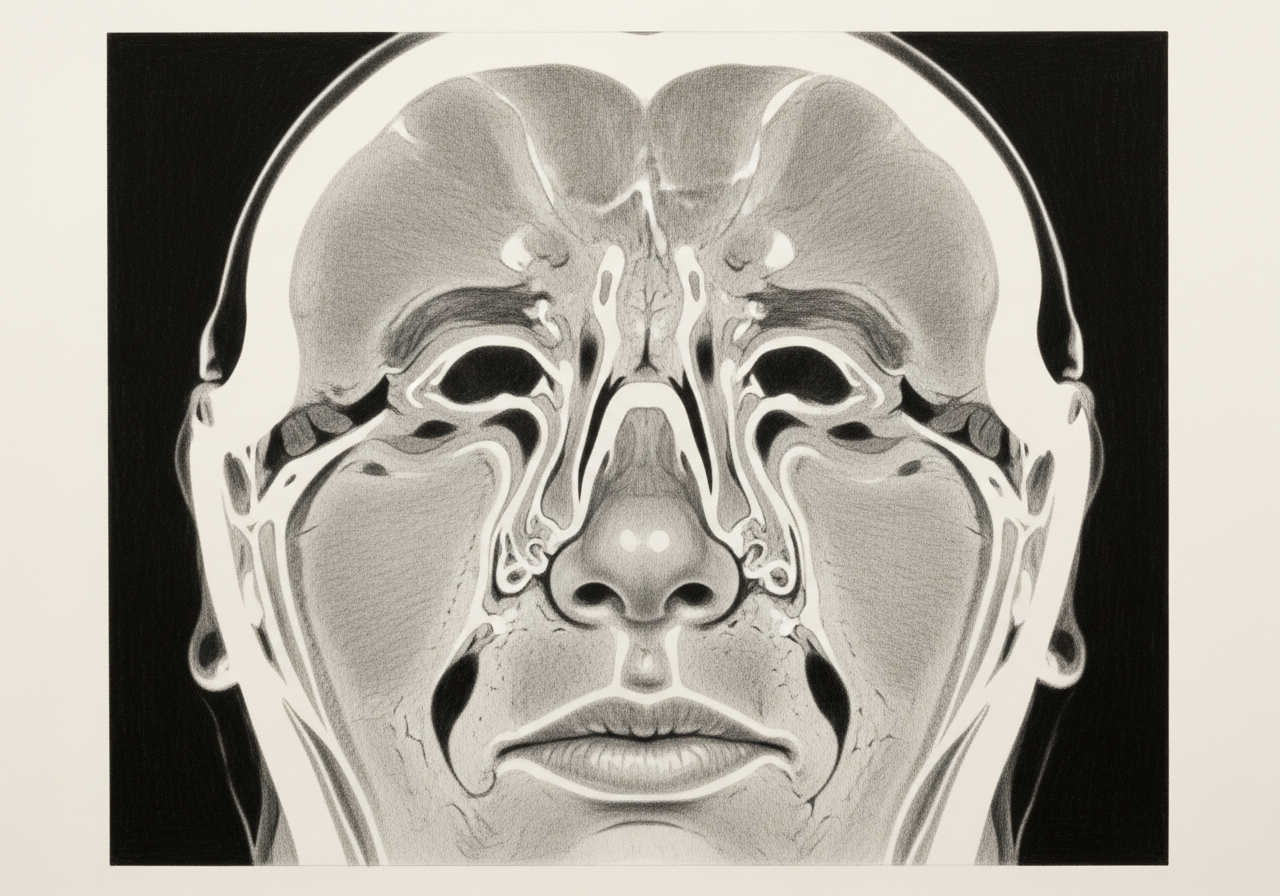
The eye sits inside a bony socket called the orbit, which shares walls with the nose and sinuses. Orbital decompression creates more space within or around the orbit by carefully removing portions of bone, fat, or both, so the eye can settle back and pressure is relieved. It is used for selected conditions, most often thyroid eye disease, as well as other compressive orbital problems.
The indication, timing, and surgical plan are individualized. They depend on vision risk, how active the underlying disease is, eye position, whether there is double vision, and a detailed ophthalmic assessment. In thyroid eye disease, surgery is often timed after the inflammation has stabilized, except when vision is threatened.
At Norelle Health, orbital decompression is planned together with ophthalmology so that the goals of surgery, the route used, and the risks are matched to each person rather than applied the same way to everyone.
What this evaluation should clarify
This page is meant to help you understand a few key decisions before considering orbital decompression:
- Whether the underlying diagnosis and the goal of treatment are established with the right examination, imaging, and testing
- How decompression compares with continued medical care, observation, radiation, or another orbital procedure
- Which factors — your anatomy, prior treatment, other health conditions, and the balance of benefits, risks, and recovery — change the recommendation
Considering orbital decompression? The next step is a quiet, unhurried conversation.
Evaluation and treatment pathway
- Confirm the diagnosis, the goal of treatment, and the reasons a less invasive or nonsurgical approach is not enough.
- Candidacy includes an ophthalmic evaluation of vision, color vision, visual fields, the optic nerve, eye movement, and the eye surface, along with a review of disease activity and CT imaging, and an agreed goal such as protecting vision or reducing bulging.
- Alternatives depend on the cause and may include medical therapy, observation, radiation, or other orbital procedures. In thyroid eye disease, the timing relative to disease activity, eye-muscle (strabismus) surgery, and eyelid surgery matters.
- An endoscopic route can decompress the inner (medial) wall and selected parts of the orbital floor through the nose, sometimes combined with external approaches. The exact walls addressed, whether fat is removed, and the balance between decompression and the risk of double vision are explained beforehand.
- Swelling, congestion, bruising, numbness, and temporary or persistent double vision can occur. Follow-up covers vision, eye movement, nasal healing, and any staged eye procedures.
Why decompression is performed
Orbital decompression is performed to make room for an eye that has been crowded forward or placed under pressure. The goals depend on the situation and may include:
- Relieving pressure on the optic nerve to protect vision
- Allowing the eyelids to close so the eye surface stays protected
- Reducing bulging (proptosis) that causes discomfort or eye exposure
- Easing pain or a feeling of pressure behind the eye
Not everyone with a prominent eye needs surgery. Many people are managed with medical therapy and observation, and decompression is reserved for selected situations.
Thyroid eye disease and other indications
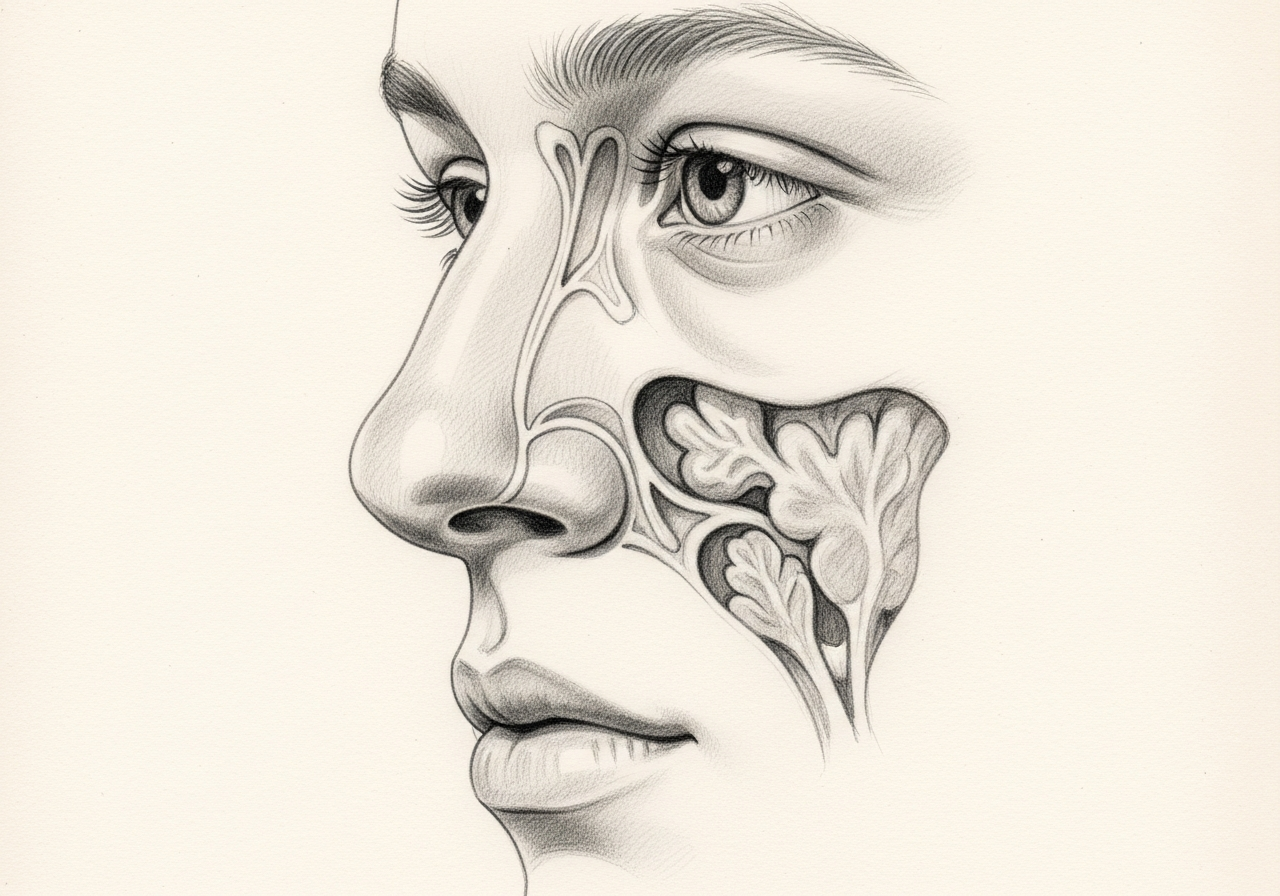
Thyroid eye disease is the most common reason for orbital decompression. In this condition, an immune process enlarges the muscles and fat behind the eye, pushing it forward. Surgery is often considered once the active, inflammatory phase has settled, unless the optic nerve is threatened and earlier decompression is needed.
Other reasons can include tumors of the orbit, certain infections that crowd the eye, and trauma. The cause influences the route, the extent of bone or fat removal, and whether other specialists are involved.
Endonasal, external and combined routes
Decompression can be approached through the nose (endonasal), through small external or eyelid incisions, or through a combination, depending on which orbital walls need to be addressed. An endoscopic endonasal route can remove the medial (inner) wall and floor of the orbit without an external scar.
In some cases, fat is removed in addition to bone. The route is chosen to address the specific area of crowding while protecting the optic nerve, the eye muscles, and nearby structures.
Double-vision and vision-risk counseling
An important part of counseling is that decompression can change eye position and alignment. New or changed double vision (diplopia) can occur after surgery and sometimes requires additional treatment, such as prisms or eye-muscle surgery, later on.
As with any surgery near the eye, there are uncommon but serious risks to vision. These risks, along with the realistic goals of surgery, are discussed in detail before proceeding so that expectations are clear.
What to bring to your consultation
Bringing the right records helps make the most of your visit. Where possible, bring or securely transfer:
- Imaging files and reports (such as CT or MRI of the orbit and sinuses)
- Any prior endoscopy or operative findings
- Pathology results, if a biopsy has been done
- Relevant laboratory results, including thyroid testing
- Notes from prior treatment and a current medication list
- The specific question you would most like answered
For complex orbital care, your records may be reviewed with the specialists involved in that part of your evaluation.
When to seek urgent care
Some symptoms need emergency assessment rather than a routine appointment. Seek immediate care for sudden vision loss, severe eye pain, rapidly increasing swelling, an inability to close the eye, heavy bleeding, a severe headache, or a neurologic change.
These can signal pressure on the optic nerve or another time-sensitive problem. An online form or routine appointment request is not an emergency service.
Medical review
This page is a patient-education resource reviewed by the responsible Norelle Health clinician before publication. It does not replace an in-person evaluation. Sudden loss of vision, rapidly worsening vision, severe eye pain, or a rapidly bulging eye should be treated as an emergency, and you should seek immediate medical care.
Specialists who perform orbital decompression

Dr. Adrian Ong
MD
Board-Certified Facial Plastic & Reconstructive and Head & Neck Surgeon
Dr. Adrian Ong is a board-certified surgeon who practices exclusively on the face, head, and neck, with expertise spanning rhinoplasty, sinus surgery, facial trauma, reconstruction, and sleep surgery.
- Functional and aesthetic rhinoplasty (including revision)
- Sinus surgery and complex revision sinus surgery
- Facial trauma and nasal fractures
- Head and neck cancer surgery and microvascular reconstruction
Also caring for this area


Not sure who to see? Our patient coordination team can help match you with the right specialist.
(212) 444-8006Frequently Asked Questions
Candidacy is based on an ophthalmic evaluation of vision, color vision, visual fields, the optic nerve, eye movement, and the eye surface, along with a review of disease activity and CT imaging, and an agreed goal such as protecting vision or reducing bulging (proptosis).
An endoscopic route can decompress the inner (medial) wall and selected parts of the orbital floor through the nose, sometimes combined with external approaches. The exact walls addressed, whether fat is removed, and the balance between decompression and the risk of double vision are explained beforehand.
Alternatives depend on the cause and may include medical therapy, observation, radiation, or other orbital procedures. In thyroid eye disease, the timing relative to disease activity, eye-muscle (strabismus) surgery, and eyelid surgery matters.
Swelling, congestion, bruising, numbness, and temporary or persistent double vision can occur. Follow-up covers vision, eye movement, nasal healing, and any staged eye procedures when relevant.
Clinical References
These independent resources from medical and professional organizations offer further reading. They are provided for general education and do not replace a consultation with a clinician.
Related Conditions

Related Procedures

1 of 2 · Endoscopic Orbital Surgery
Request a consultation about orbital decompression
Schedule a consultation with our team to discuss whether this procedure is the right option for you.