

Overview
Most nosebleeds stop with correct pressure, but recurrent, heavy, or one-sided bleeding can reflect dryness, medication effects, blood-pressure or clotting issues, trauma, vascular lesions, or tumors. Care leads with safe first aid and then explains when endoscopy, cautery, packing, laboratory evaluation, or hospital care is appropriate.
What this evaluation should clarify
A focused evaluation should help you understand a few key decisions:
- What objective evidence distinguishes epistaxis from look-alike conditions
- Which anatomic, inflammatory, dental, neurologic, infectious, or tumor-related contributors must be considered
- Which medical, procedural, surgical, or multidisciplinary path fits the findings and your goals
Living with epistaxis and nosebleeds? The next step is a quiet, unhurried conversation.
Evaluation and treatment pathway
- Clarify the symptom pattern, duration, triggers, prior treatment, operations, medications, and relevant medical history.
- Evaluation considers bleeding severity and laterality, medication and anticoagulant use, trauma, blood pressure, anemia or clotting risk, and nasal examination. Recurrent unilateral bleeding may warrant endoscopy and targeted imaging.
- Identify important look-alikes, complications, and contributors before assigning a definitive diagnosis.
- Initial treatment uses firm, continuous pressure in the correct location. Moisturization, topical treatment, cautery, packing, medication coordination, arterial procedures, or treatment of a focal cause may follow according to severity and findings.
- Set a measurable follow-up plan: symptom goals, objective reassessment, medication response, and imaging or surveillance when appropriate.
Causes and risk factors
Common causes include dry air, nose rubbing or picking, allergies, colds, and minor injury. Blood-thinning medications, aspirin, high blood pressure, and bleeding disorders can make nosebleeds more frequent or harder to control.
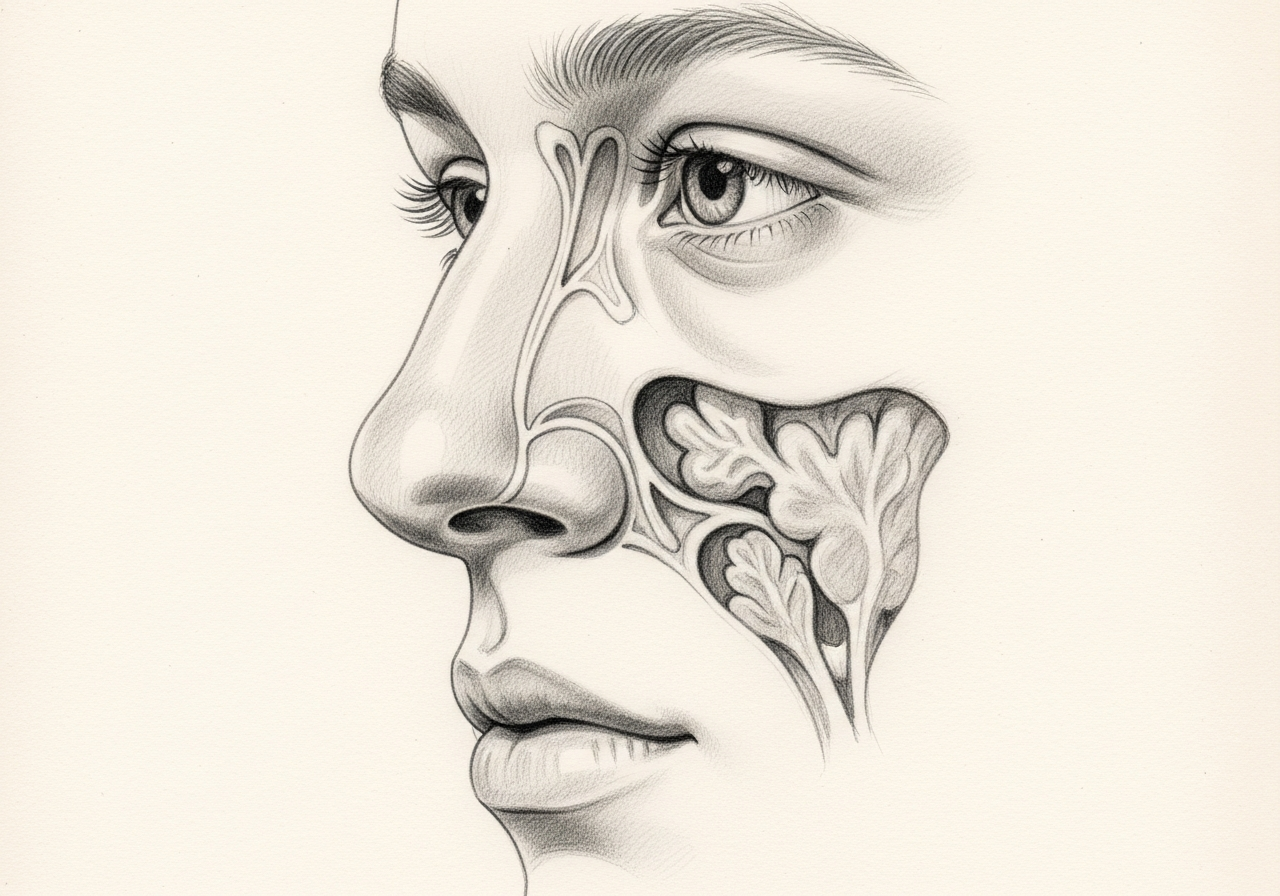
Less commonly, recurrent one-sided bleeding can be associated with a growth in the nose and deserves evaluation.
First aid and what to do
For most nosebleeds, sit upright, lean slightly forward, and pinch the soft part of the nose just below the bony bridge for ten to fifteen minutes without releasing. Leaning forward helps keep blood from draining into the throat.
Applying a cold compress and avoiding nose blowing afterward can help. If bleeding does not stop after sustained pressure, seek medical care.
Treatment options
Treatment is matched to the source and severity:
- Nasal saline, humidification, and moisturizing ointment to prevent dryness
- Cautery of a visible bleeding vessel
- Nasal packing to control active bleeding
- Review of blood-thinning medications with the prescribing clinician
- Procedures to control posterior bleeding in selected cases
Preventing dryness and avoiding trauma to the nose are important for reducing recurrence.
What to bring to your consultation
Bringing or securely transferring the records that can change this decision helps make the visit productive:
- Imaging files and reports
- Endoscopy or operative findings
- Pathology results
- Laboratory results
- Prior treatment notes
- A current medication list
- The specific question you want answered
When to seek urgent care
Emergency care is appropriate when bleeding is heavy, compromises breathing, follows major trauma, causes faintness or marked weakness, continues despite sustained correct pressure, or occurs with signs of major blood loss. Do not drive if unstable.
Medical review
This page is a patient-education resource reviewed by the responsible Norelle Health clinician before publication. It does not replace an in-person evaluation. If symptoms are severe or rapidly worsening, seek immediate medical care.
Specialists who treat epistaxis and nosebleeds

Dr. Adrian Ong
MD
Board-Certified Facial Plastic & Reconstructive and Head & Neck Surgeon
Dr. Adrian Ong is a board-certified surgeon who practices exclusively on the face, head, and neck, with expertise spanning rhinoplasty, sinus surgery, facial trauma, reconstruction, and sleep surgery.
- Functional and aesthetic rhinoplasty (including revision)
- Sinus surgery and complex revision sinus surgery
- Facial trauma and nasal fractures
- Head and neck cancer surgery and microvascular reconstruction
Also caring for this area


Not sure who to see? Our patient coordination team can help match you with the right specialist.
(212) 444-8006Frequently Asked Questions
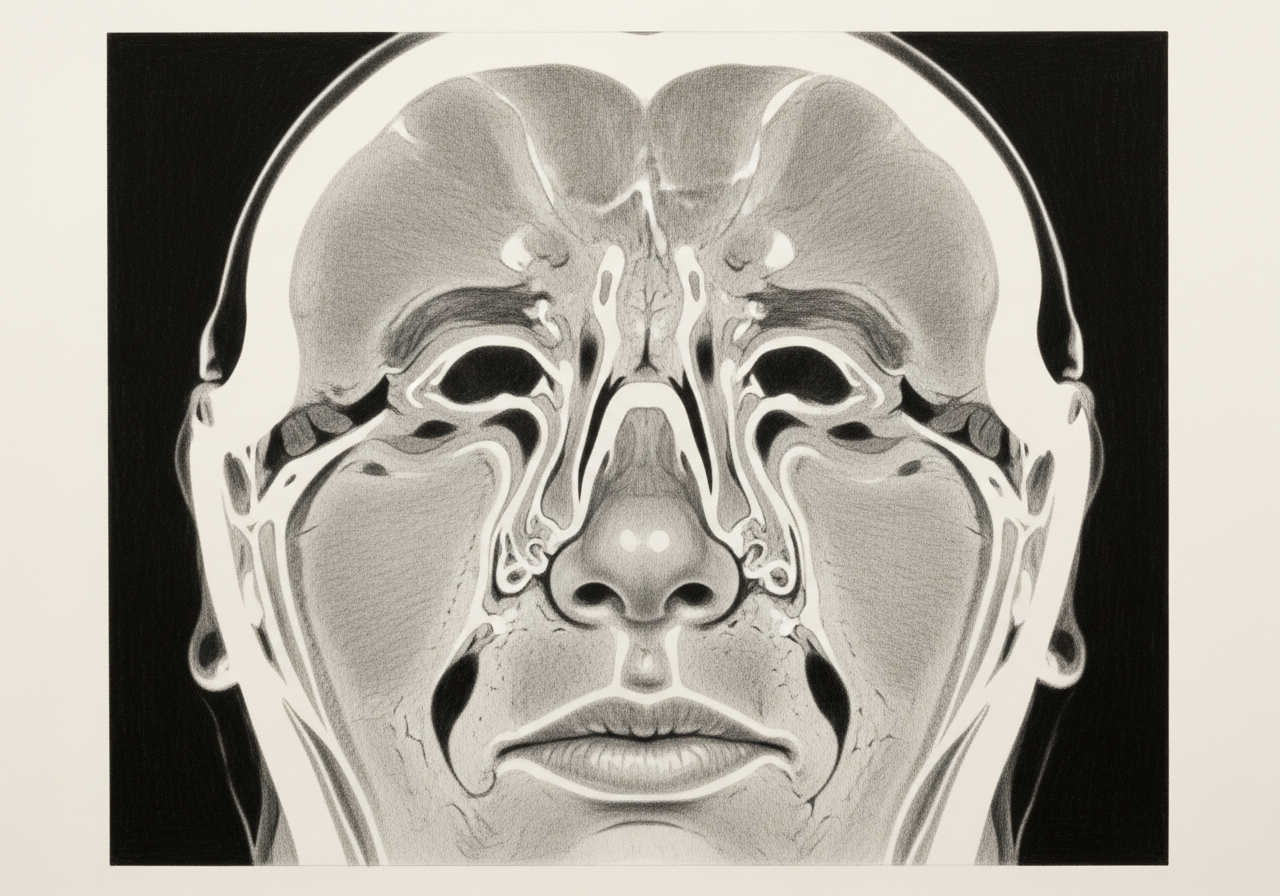
Epistaxis is bleeding from the nasal lining. It may arise from an anterior surface vessel or a deeper posterior source and can be influenced by dryness, trauma, medication, systemic disease, or a focal lesion.
Evaluation considers bleeding severity and laterality, medication and anticoagulant use, trauma, blood pressure, anemia or clotting risk, and nasal examination. Recurrent unilateral bleeding may warrant endoscopy and targeted imaging.
Initial treatment uses firm, continuous pressure in the correct location. Moisturization, topical treatment, cautery, packing, medication coordination, arterial procedures, or treatment of a focal cause may follow according to severity and findings.
Emergency care is appropriate when bleeding is heavy, compromises breathing, follows major trauma, causes faintness or marked weakness, continues despite sustained correct pressure, or occurs with signs of major blood loss. Do not drive if unstable.
Clinical References
These independent resources from medical and professional organizations offer further reading. They are provided for general education and do not replace a consultation with a clinician.
Related Conditions

1 of 4 · Juvenile Nasopharyngeal Angiofibroma
Request a consultation for epistaxis and nosebleeds
Schedule an evaluation with our team to review your symptoms and the appropriate next steps.