

Overview
A suspected skull-base fracture is a trauma emergency, not an elective office diagnosis. Acute injuries need emergency care first. Specialist follow-up then addresses cerebrospinal-fluid leakage, smell loss, cranial-nerve injury, hearing or balance symptoms, infection risk, and reconstruction.
What this evaluation should clarify
After emergency care, focused follow-up should help you understand a few key decisions:
- What objective evidence distinguishes a skull base fracture from look-alike conditions
- Which anatomic, inflammatory, dental, neurologic, infectious, or tumor-related contributors must be considered
- Which medical, procedural, surgical, or multidisciplinary path best fits the findings and your goals
Living with skull base fracture? The next step is a quiet, unhurried conversation.
Evaluation and treatment pathway
- Clarify the symptom pattern, duration, triggers, prior treatment, operations, medications, and relevant medical history.
- Acute evaluation occurs in a hospital trauma setting with neurologic assessment and appropriate CT, with MRI, vascular imaging, hearing, vision, or cranial-nerve testing selected according to the injury. Clear drainage may require CSF-specific laboratory testing.
- Identify important look-alikes, complications, and contributors before assigning a definitive diagnosis.
- Many fractures are managed nonoperatively with hospital observation and complication monitoring, while persistent leaks, displaced defects, vascular injury, compression, or other complications may require targeted intervention.
- Set a measurable follow-up plan: symptom goals, objective reassessment, medication response, and imaging or surveillance when appropriate.
Symptoms
Signs can include clear, watery drainage from the nose or ear, bruising around the eyes or behind the ear, hearing changes, dizziness, and a reduced sense of smell. Facial weakness, numbness, or vision changes may occur depending on which nerves are affected.
Clear nasal or ear drainage after head trauma is particularly important because it can indicate a cerebrospinal fluid leak.
Causes and risk factors
Skull base fractures result from high-energy head trauma, such as motor vehicle crashes, falls from height, sports injuries, or assaults. The pattern of the fracture depends on the direction and force of the impact.
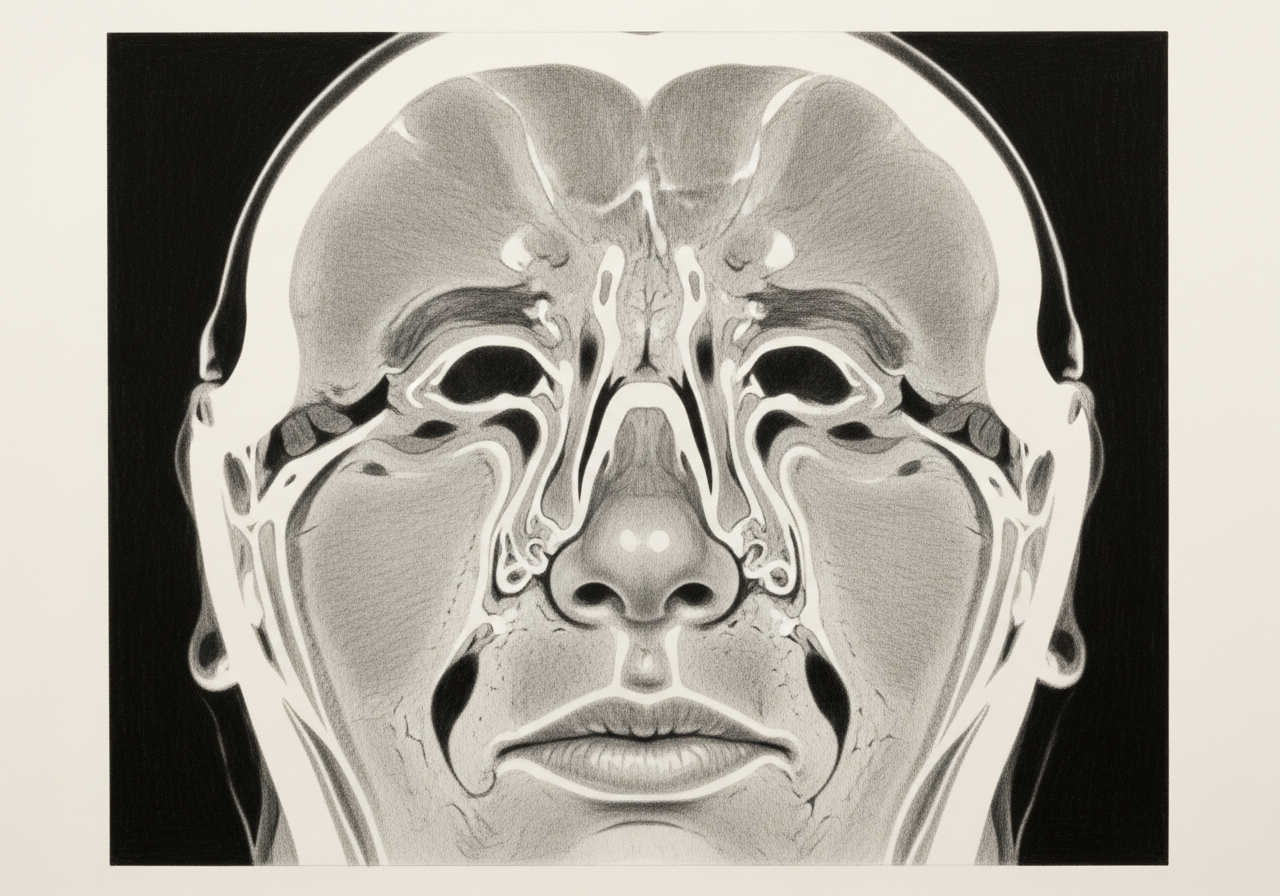
The main concern beyond the fracture itself is injury to the nerves, vessels, ears, and the barrier between the nose and the brain.
How it is diagnosed
CT imaging is the primary tool for diagnosing skull base fractures and is usually performed during emergency evaluation. When a cerebrospinal fluid leak is suspected, nasal fluid can be tested for beta-2 transferrin, a protein specific to cerebrospinal fluid.
Nasal endoscopy and additional imaging help locate any defect and plan repair if one is needed.
Treatment options
Treatment depends on the fracture and its complications:
- Emergency stabilization and CT imaging
- Observation, because many stable fractures heal without surgery
- Monitoring and management of a cerebrospinal fluid leak
- Endoscopic repair of skull-base defects or CSF leaks
- Treatment of associated nerve or sinus injuries
- Neurosurgery collaboration when appropriate
Many cerebrospinal fluid leaks at the skull base can be repaired endoscopically through the nose, avoiding external incisions.
What to bring to your consultation
Bringing or securely transferring the records that can change this decision helps make the visit productive:
- Imaging files and reports
- Endoscopy or operative findings
- Pathology results
- Laboratory results
- Prior treatment notes
- A current medication list
- The specific question you want answered
When to seek urgent care
After head trauma, loss of consciousness, repeated vomiting, worsening headache, confusion, weakness, seizure, major bleeding, clear nasal or ear drainage, vision change, facial weakness, or severe neck pain requires emergency care.
Medical review
This page is a patient-education resource reviewed by the responsible Norelle Health clinician before publication. It does not replace an in-person evaluation. If symptoms are severe or rapidly worsening, seek immediate medical care.
Specialists who treat skull base fracture

Dr. Adrian Ong
MD
Board-Certified Facial Plastic & Reconstructive and Head & Neck Surgeon
Dr. Adrian Ong is a board-certified surgeon who practices exclusively on the face, head, and neck, with expertise spanning rhinoplasty, sinus surgery, facial trauma, reconstruction, and sleep surgery.
- Functional and aesthetic rhinoplasty (including revision)
- Sinus surgery and complex revision sinus surgery
- Facial trauma and nasal fractures
- Head and neck cancer surgery and microvascular reconstruction
Also caring for this area


Not sure who to see? Our patient coordination team can help match you with the right specialist.
(212) 444-8006Frequently Asked Questions
A skull-base fracture is a break in the bone separating the cranial cavity from the sinuses, ears, orbit, or upper neck and may involve nerves, vessels, or a cerebrospinal-fluid leak.
Acute evaluation occurs in a hospital trauma setting with neurologic assessment and appropriate CT, with MRI, vascular imaging, hearing, vision, or cranial-nerve testing selected according to the injury. Clear drainage may require CSF-specific laboratory testing.
Many fractures are managed nonoperatively with hospital observation and complication monitoring, while persistent leaks, displaced defects, vascular injury, compression, or other complications may require targeted intervention.
After head trauma, loss of consciousness, repeated vomiting, worsening headache, confusion, weakness, seizure, major bleeding, clear nasal or ear drainage, vision change, facial weakness, or severe neck pain requires emergency care.
Clinical References
These independent resources from medical and professional organizations offer further reading. They are provided for general education and do not replace a consultation with a clinician.
Related Procedures

1 of 2 · Skull Base Fracture Repair
Related Conditions

Request a consultation for skull base fracture
Schedule an evaluation with our team to review your symptoms and the appropriate next steps.