

Overview
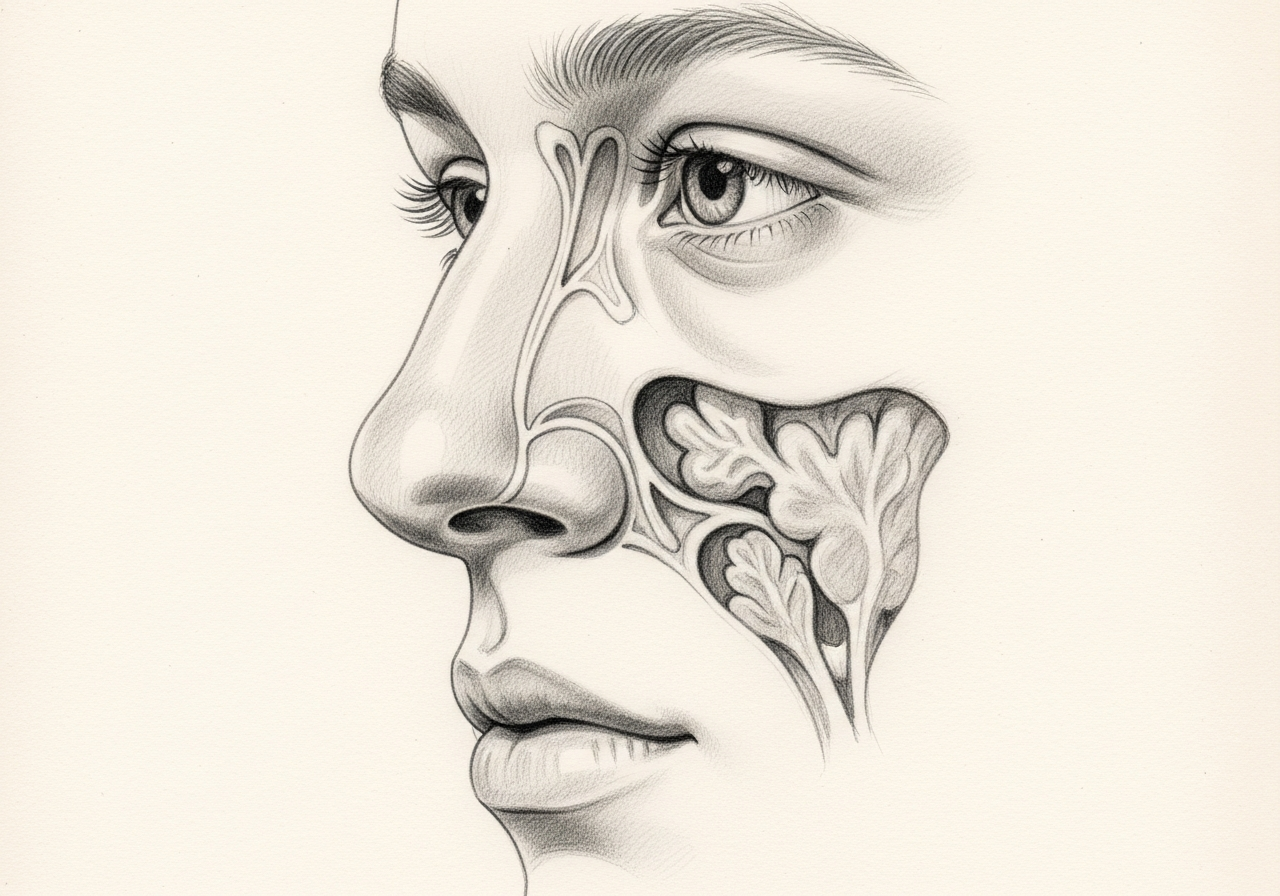
Nasal cavity and sinus cancers are uncommon and biologically diverse. The treatment plan should begin with expert pathology and imaging review, then account for the exact subsite, orbit and skull-base involvement, neck or distant spread, resectability, radiation or systemic therapy, and the functions treatment may affect.
What this evaluation should clarify
A focused evaluation should help you understand a few key decisions:
- What objective evidence distinguishes a sinonasal cancer from look-alike conditions
- Which anatomic, inflammatory, dental, neurologic, infectious, or tumor-related contributors must be considered
- Which medical, procedural, surgical, or multidisciplinary path best fits the findings and your goals
Living with nasal and sinus cancer? The next step is a quiet, unhurried conversation.
Evaluation and treatment pathway
- Clarify the symptom pattern, duration, triggers, prior treatment, operations, medications, and relevant medical history.
- Evaluation includes endoscopy, biopsy, and pathology review, CT and MRI for local extent, and staging studies selected according to tumor type. Dental, vision, cranial-nerve, and neck assessment may be relevant.
- Identify important look-alikes, complications, and contributors before assigning a definitive diagnosis.
- Treatment can involve endoscopic, open, or combined surgery, radiation, systemic therapy, or combinations. Reconstruction, eye preservation, skull-base closure, and functional rehabilitation should be planned before definitive treatment when relevant.
- Set a measurable follow-up plan: symptom goals, objective reassessment, medication response, and imaging or surveillance when appropriate.
Symptoms
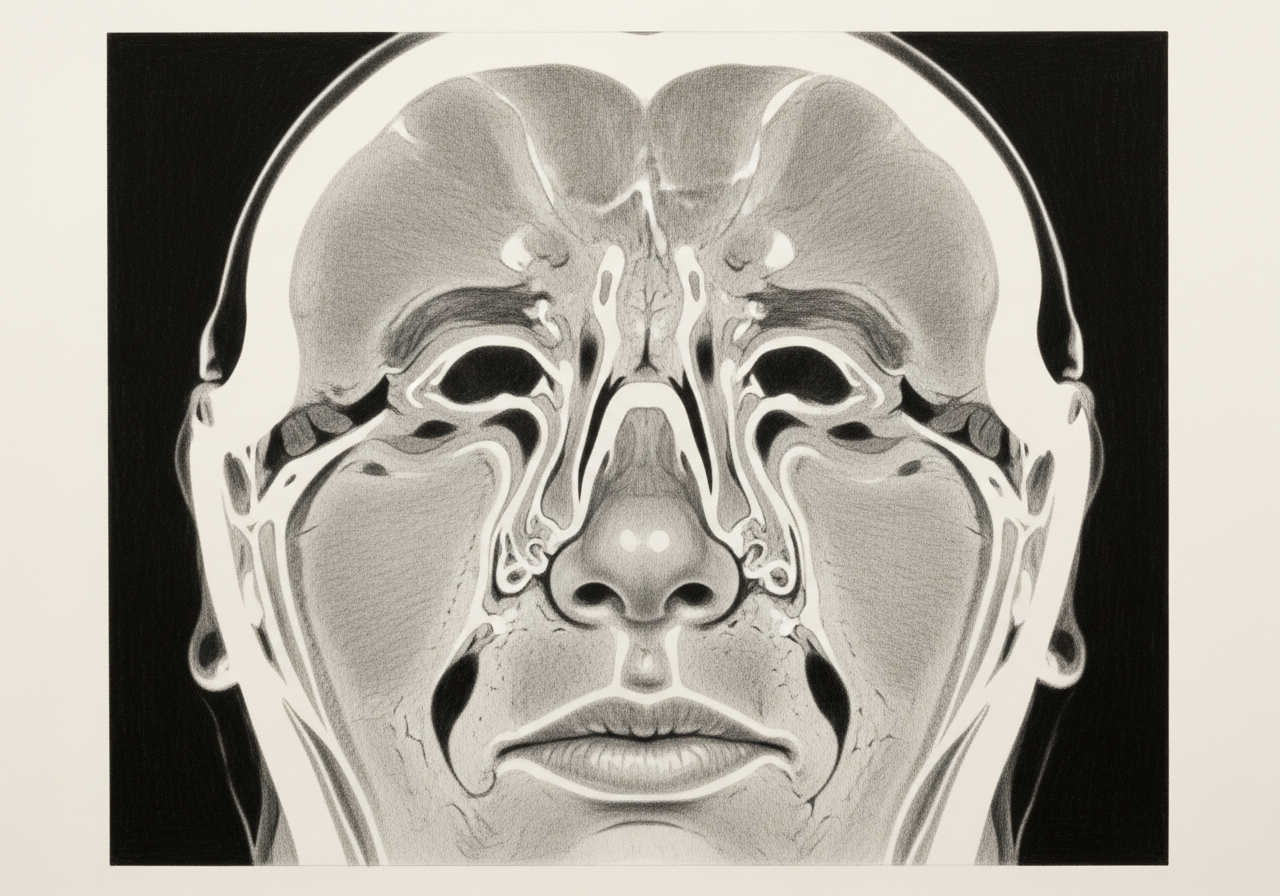
Common symptoms include nasal blockage on one side, recurrent nosebleeds, facial pain or numbness, a reduced sense of smell, and nasal drainage that does not clear. As a tumor grows, it may cause eye changes such as bulging, double vision, or tearing, or loosening of the upper teeth.
Many of these symptoms have benign causes, but the combination of one-sided, persistent, and treatment-resistant symptoms should prompt a focused examination.
Causes and risk factors
The exact cause is often unknown. Recognized risk factors can include long-term occupational exposure to wood dust, leather dust, nickel, or certain chemical fumes, as well as tobacco use. Some sinonasal tumors are associated with human papillomavirus or with prior inverted papilloma.
Having a risk factor does not mean cancer will develop, and many people with sinonasal cancer have no identifiable exposure.
How it is diagnosed
Evaluation begins with a history and nasal endoscopy, which lets the clinician inspect areas not visible on a routine exam. CT and MRI imaging help define the size and extent of a tumor and whether it involves the eye socket or skull base.
A biopsy is needed to confirm the diagnosis and identify the tumor type. When a malignancy is confirmed, care is typically coordinated through a multidisciplinary team.
Treatment options
Treatment is individualized to the tumor type, location, and extent, and may combine more than one approach:
- Surgery, often endoscopic, to remove the tumor when feasible
- Open surgical approaches for more extensive tumors
- Radiation therapy
- Chemotherapy or other systemic therapy
- Reconstruction and rehabilitation
- Neurosurgery collaboration when the skull base is involved
The plan is developed with the patient and the treating team, with attention to preserving function such as breathing and vision when possible.
What to bring to your consultation
Bringing or securely transferring the records that can change this decision helps make the visit productive:
- Imaging files and reports
- Endoscopy or operative findings
- Pathology results
- Laboratory results
- Prior treatment notes
- A current medication list
- The specific question you want answered
When to seek urgent care
Major bleeding, breathing difficulty, acute vision loss, rapidly increasing eye swelling, severe headache, new neurologic symptoms, or inability to maintain hydration requires urgent or emergency care.
Medical review
This page is a patient-education resource reviewed by the responsible Norelle Health clinician before publication. It does not replace an in-person evaluation. If symptoms are severe or rapidly worsening, seek immediate medical care.
Specialists who treat nasal and sinus cancer

Dr. Adrian Ong
MD
Board-Certified Facial Plastic & Reconstructive and Head & Neck Surgeon
Dr. Adrian Ong is a board-certified surgeon who practices exclusively on the face, head, and neck, with expertise spanning rhinoplasty, sinus surgery, facial trauma, reconstruction, and sleep surgery.
- Functional and aesthetic rhinoplasty (including revision)
- Sinus surgery and complex revision sinus surgery
- Facial trauma and nasal fractures
- Head and neck cancer surgery and microvascular reconstruction
Also caring for this area


Not sure who to see? Our patient coordination team can help match you with the right specialist.
(212) 444-8006Frequently Asked Questions
Sinonasal cancer includes malignant tumors arising in the nasal cavity or paranasal sinuses, with treatment and prognosis varying substantially by histology, site, and stage.
Evaluation includes endoscopy, biopsy, and pathology review, CT and MRI for local extent, and staging studies selected according to tumor type. Dental, vision, cranial-nerve, and neck assessment may be relevant.
Treatment can involve endoscopic, open, or combined surgery, radiation, systemic therapy, or combinations. Reconstruction, eye preservation, skull-base closure, and functional rehabilitation should be planned before definitive treatment when relevant.
Major bleeding, breathing difficulty, acute vision loss, rapidly increasing eye swelling, severe headache, new neurologic symptoms, or inability to maintain hydration requires urgent or emergency care.
Clinical References
These independent resources from medical and professional organizations offer further reading. They are provided for general education and do not replace a consultation with a clinician.
Related Procedures

1 of 2 · Endoscopic Skull Base Surgery
Related Conditions

1 of 3 · Inverted Papilloma and Sinonasal Tumors
Request a consultation for nasal and sinus cancer
Schedule an evaluation with our team to review your symptoms and the appropriate next steps.