

Overview
An adult neck mass without a clear infectious cause should be treated as potentially serious until a diagnosis is established, and a lump present for two weeks or longer without significant fluctuation, or of uncertain duration, meets a guideline threshold for malignancy-risk assessment.
A neck mass is any lump or swelling in the neck. The neck contains lymph nodes, the thyroid and parathyroid glands, salivary glands, blood vessels, nerves, and developmental remnants, so a mass can arise from many of these structures.
Many neck masses are benign, such as a reactive lymph node from an infection or a simple cyst. However, a neck mass in an adult present for two weeks or longer, or of uncertain duration, should be evaluated, because a small number represent something more significant, including head and neck cancer. The location, how long it has been present, and accompanying symptoms all help narrow the cause.
Norelle Health evaluates neck masses with a careful history, examination, and imaging, often starting with ultrasound, and uses fine needle aspiration when tissue sampling is needed. Care is coordinated with radiology and pathology so the diagnosis is established before any treatment decision.
How we approach the decision
The aim is to reach a diagnosis efficiently and to avoid the delay that comes from treating an undiagnosed mass empirically. The decisions this page is meant to help you understand are:
- Is there a convincing infectious cause, or has empiric treatment delayed diagnosis?
- What do the mass location, consistency, imaging, and symptoms suggest about a thyroid, salivary, lymph-node, congenital, or other origin?
- Can fine needle aspiration establish the diagnosis without an open biopsy?

Living with neck mass? The next step is a quiet, unhurried conversation.
What happens next
Evaluation usually follows a clear sequence:
- A complete head and neck examination, including the skin and cranial nerves.
- Flexible endoscopy when an upper aerodigestive source is possible.
- Contrast imaging or ultrasound based on the suspected origin, the same starting point used in a thyroid nodule evaluation or a parotid tumor specialist assessment when those glands are the likely source.
- Fine needle aspiration rather than open biopsy for most undiagnosed adult neck masses.
- Continued evaluation of cystic masses until a definitive diagnosis is reached, since a cystic adult mass can represent head and neck cancer, including an unknown primary head and neck cancer.
Symptoms and warning signs
A neck mass may be painless or tender, soft or firm, and stable or growing. Reactive lymph nodes from a cold are common and usually settle within a few weeks.
Warning signs that deserve prompt evaluation include a mass that persists for two weeks or longer, is firm or fixed, is enlarging, or occurs with a sore throat, voice change, swallowing difficulty, one-sided ear pain, or unexplained weight loss, especially in adults who smoke.
Causes and risk factors
Common causes of a neck mass include:
- Reactive or infected lymph nodes
- Congenital cysts such as branchial cleft or thyroglossal duct cysts
- Thyroid nodules or an enlarged thyroid
- Salivary gland swelling or stones
- Benign tumors
- Less often, lymphoma or metastatic head and neck cancer
Risk factors a clinician may ask about include age, tobacco and alcohol use, and recent infections.
How it is diagnosed
Evaluation begins with a history and a careful neck examination, including the location, size, and character of the mass. Imaging and sampling follow as needed:
- Ultrasound is often the first imaging study
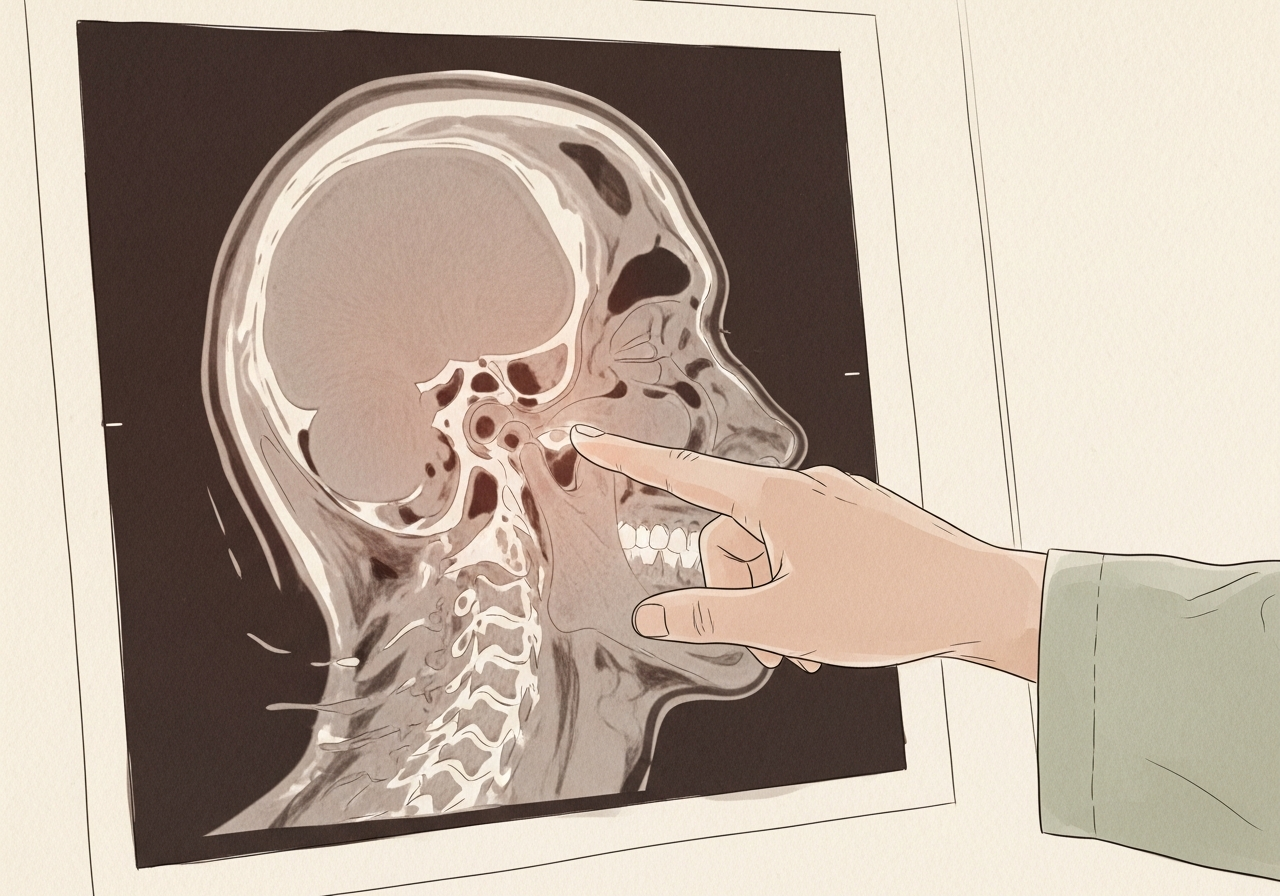
- CT or MRI may be used for deeper or larger masses
- Fine needle aspiration provides a tissue diagnosis
- Flexible endoscopy examines the throat when cancer is a concern
The aim is to reach a clear diagnosis before treatment.
Treatment options
Treatment depends entirely on the cause. A reactive lymph node may simply be observed, while an infected node or cyst may be treated with antibiotics.
Thyroid, salivary gland, and congenital masses are managed according to their specific diagnosis, and surgery is used when removal is appropriate. When a mass represents cancer, care is coordinated with the appropriate oncology and surgical teams. The plan follows the diagnosis rather than the lump alone.

Needle biopsy
Fine needle aspiration is often the first tissue test for a suspicious neck mass because it can sample cells without an open incision, usually with ultrasound guidance. A core biopsy may be used in selected situations, and the specimen is handled differently depending on whether the suspected source is the thyroid, a salivary gland, lymphoma, or a squamous cancer.
An open biopsy is generally not the first step for a neck node that may be metastatic, because it can complicate later treatment. The right approach is chosen after examination and imaging.
When the primary tumor is not found
When a lymph node contains cancer but the original site is not visible, evaluation may include detailed imaging, endoscopy under anesthesia, directed biopsies, and assessment of the tonsils and base of the tongue. Pathology testing can help suggest an HPV-related or other origin, and treatment is individualized to the likely site and lymph node stage.
When to seek urgent care
Use these categories to guide timing:
- Emergency, meaning call 911 or go to the nearest emergency department: difficulty breathing, an inability to swallow, significant bleeding, or rapidly increasing swelling with severe infection signs.
- Same-day or urgent evaluation: facial weakness, a voice change, progressive swallowing trouble, weight loss, or a quickly enlarging mass.
- Routine specialist evaluation: any adult neck mass that persists for two weeks or longer or is of uncertain duration, even when it looks benign.
The online consultation form is for routine scheduling and is not an emergency service.
Clinical perspective
Our head and neck surgeons treat the adult neck mass as one of the division's highest-priority symptoms, because losing time to repeated antibiotic courses can delay an important diagnosis. The location of the mass — under the jaw, along the side of the neck, in the midline, in the thyroid bed, behind the ear or in the parotid, or above the collarbone — helps narrow the likely source.
Factors that raise concern include a firm or fixed mass, steady growth, a cystic mass in an adult, a history of tobacco or alcohol use, and associated symptoms such as a voice change or swallowing difficulty. A clearly reactive node during an active infection is a factor that may reasonably be observed for a short, defined interval.
What commonly changes the recommendation is the result of imaging and fine needle aspiration and whether endoscopy identifies a primary site. Candidacy for any procedure is determined individually after specialist review rather than from the lump alone.
What to bring to your consultation
Bringing the right records makes a consultation more efficient. Helpful items include:
- Prior imaging and the written reports
- Pathology or biopsy results when available
- Recent laboratory results
- Treatment notes from any prior care
- A current medication list
- The specific decision you want the consultation to answer
Request a consultation for a focused review of the diagnosis, the available options, the likely tradeoffs, and the steps needed before treatment. For urgent symptoms, follow the guidance above rather than using the routine form.
Medical review
This page is a patient-education resource reviewed by the responsible Norelle Health clinician before publication. It does not replace an in-person evaluation. If symptoms are severe or rapidly worsening, seek immediate medical care.
Specialists who treat neck mass

Dr. Moustafa Mourad
MD, FACS
Double Board-Certified Head & Neck and Facial Plastic & Reconstructive Surgeon
Dr. Moustafa Mourad is a double board-certified head and neck and facial plastic and reconstructive surgeon who cares for the full range of cosmetic and complex conditions affecting the face, head, and neck.
- Facial plastic and reconstructive surgery
- Head and neck cancer surgery
- Microvascular free-flap reconstruction
- Facial trauma and reconstruction
Also caring for this area


Not sure who to see? Our patient coordination team can help match you with the right specialist.
(212) 444-8006Frequently Asked Questions
Common causes include enlarged or infected lymph nodes, cysts, thyroid nodules, and salivary gland problems. Less often, a neck mass represents lymphoma or head and neck cancer, which is why evaluation matters.
Any neck mass in an adult present for two weeks or longer, or of uncertain duration, should be evaluated, and sooner if it is enlarging or firm or occurs with a voice change, swallowing trouble, ear pain, or weight loss.
A mass present for two weeks or longer without significant fluctuation, or of uncertain duration, should be assessed for malignancy risk when there is no clear infectious cause.
Fine needle aspiration can often establish a diagnosis with less disruption. An open biopsy may complicate later cancer treatment and is generally not the first diagnostic step for an undiagnosed adult neck mass.
Yes. Although congenital cysts occur, a cystic adult neck mass can represent metastatic HPV-related or other cancer and should not be assumed benign without evaluation.
Evaluation usually includes a history, a neck examination, and ultrasound. CT or MRI may be added for deeper masses, and fine needle aspiration provides a tissue diagnosis when needed.
No. Many neck masses are benign, such as reactive lymph nodes or cysts. The purpose of evaluation is to identify the smaller number that need further treatment.
It is an office-based test that uses a thin needle, often guided by ultrasound, to sample cells from the mass for analysis. It helps determine whether a mass is benign, suspicious, or unclear.
Antibiotics are appropriate when a bacterial infection is genuinely suspected. Taking repeated courses without a clear infection can delay the diagnosis of other causes, so a persistent mass should be evaluated.
Most needle biopsies are brief and performed with local measures, and ultrasound guidance can improve targeting. Discomfort varies from person to person.
Yes. HPV-related oropharyngeal cancer can present as an enlarged neck node, sometimes with mild or no throat symptoms. Because a neck mass has many possible causes, evaluation is needed rather than assuming a diagnosis.
No. Many are observed or treated medically. Surgery is used when the diagnosis or symptoms make removal appropriate, based on the specific cause.
Because a small number of persistent neck masses in adults represent head and neck cancer or lymphoma. Evaluation distinguishes benign causes from those that need treatment.
Clinical References
These independent resources from medical and professional organizations offer further reading. They are provided for general education and do not replace a consultation with a clinician.
Related Procedures

Related Conditions

1 of 6 · Unknown Primary Head and Neck Cancer
Request a consultation for neck mass
Schedule an evaluation with our team to review your symptoms and the appropriate next steps.