

About the Procedure
Persistent symptoms after sinus surgery do not automatically mean another operation is needed. A revision evaluation should reconstruct the original diagnosis and operation, review imaging and pathology, identify scar or residual anatomy, reassess inflammatory disease, and define the specific problem a second procedure would solve.
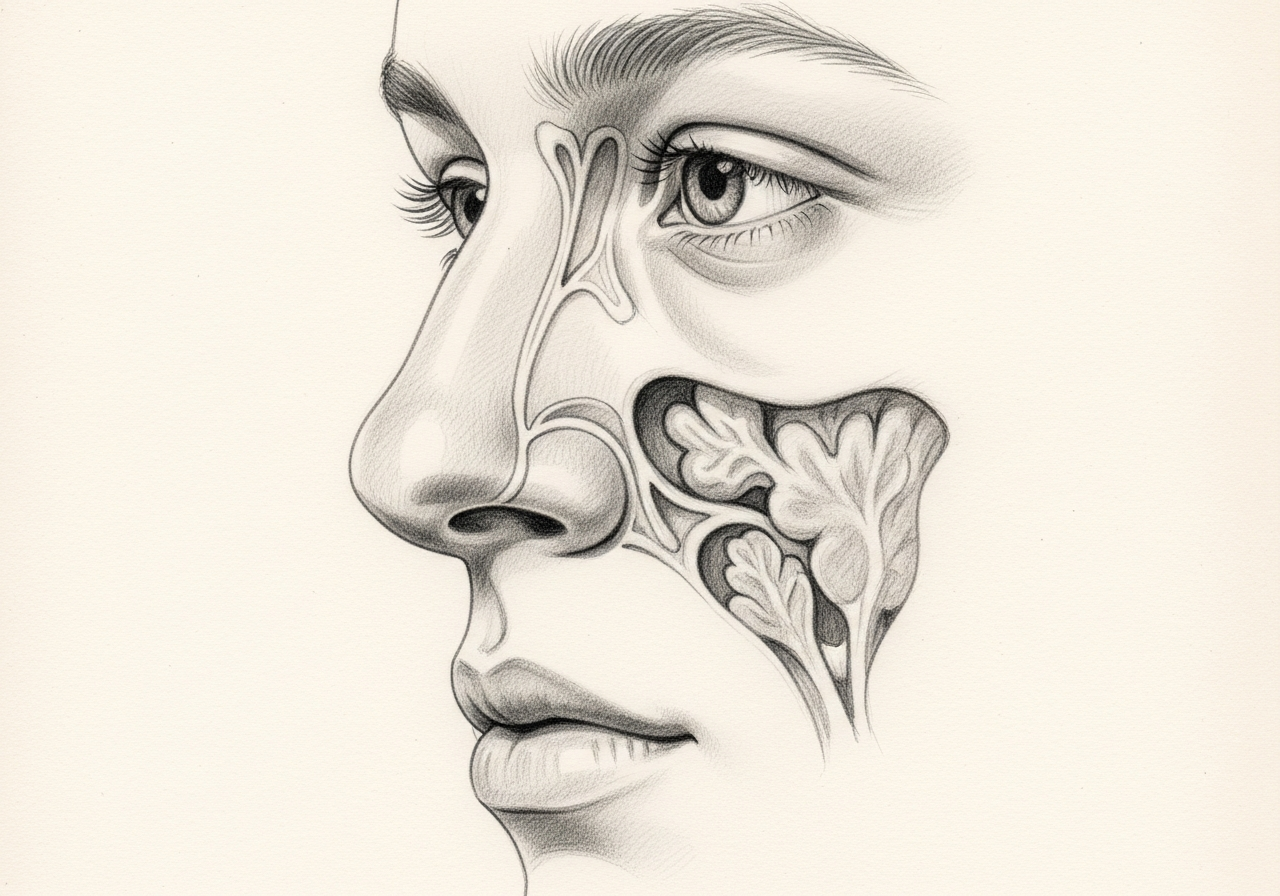
Persistent disease can result from scar tissue, retained bony partitions, recurrent polyps, ongoing inflammation, or areas that were not fully addressed at the first surgery. Because anatomy is often altered after prior surgery, revision cases require careful re-evaluation that includes nasal endoscopy, review of prior CT imaging and operative reports, and an assessment of underlying inflammatory or allergic conditions.
What this evaluation should clarify
A revision evaluation should clarify a few core questions:
- Is the underlying diagnosis and treatment goal established with the right examination, imaging, testing, or pathology?
- How does this option compare with continued medical care, a different procedure, observation, or referral to another specialty?
- Which anatomy, prior treatment, comorbidities, benefits, risks, and recovery requirements change the recommendation?
Considering revision sinus surgery? The next step is a quiet, unhurried conversation.
Evaluation and treatment pathway
- Confirm the diagnosis, treatment goal, and the reasons a less invasive or nonsurgical approach is insufficient.
- Candidacy requires prior operative notes, imaging files, pathology, medication history, and a fresh endoscopic examination. The evaluation should separate persistent sinus disease from migraine, rhinitis, neuropathic pain, dental disease, or other explanations for ongoing symptoms.
- Alternatives may include optimized topical delivery, biologic treatment, management of asthma, AERD, or allergy, dental care, headache referral, observation, or a targeted rather than broad revision.
- The operation is individualized to distorted anatomy and the identified failure mechanism. It may address scarring, retained partitions, blocked frontal or sphenoid pathways, recurrent polyps, mucoceles, or other defined disease, often with navigation.
- Recovery may resemble primary sinus surgery but varies with extent, scarring, and reconstruction. Frequent early follow-up, debridement, and long-term inflammatory control can be particularly important.
How it is performed
The procedure is performed through the nostrils using endoscopes, often with image guidance because anatomy is altered after prior surgery. The surgeon removes scar tissue, opens or enlarges blocked drainage pathways, removes recurrent polyps, and addresses partitions that limit access.
The extent is tailored to the findings, and healthy tissue is preserved to reduce further scarring.
Risks and alternatives
Risks are similar to initial sinus surgery, including bleeding, infection, crusting, recurrent scarring, persistent symptoms, and changes in smell. Because of altered anatomy, there can be slightly higher risk near the eye and skull base, which the team works carefully to avoid.
Alternatives include optimized medical therapy, allergy management, and treatment of conditions such as aspirin-exacerbated respiratory disease. Surgery is recommended when these are not enough and findings support it.
Results and follow-up
Revision surgery aims to restore drainage, remove recurrent disease, and improve access for topical medication. Because recurrence is often driven by an underlying inflammatory tendency, ongoing medical therapy and follow-up are important to maintain results.
Regular endoscopy helps detect early scarring or recurrence so it can be managed before it causes major problems.
What to bring to your consultation
Bring or securely transfer the records that can change this decision:
- Imaging files and reports, including prior sinus CT
- Endoscopy or operative findings from previous surgery
- Pathology results
- Laboratory results and allergy testing
- Prior treatment notes
- A current medication list
- The specific question you want answered
A timeline of your symptoms also helps separate persistent sinus disease from other causes of ongoing symptoms.
When to seek urgent care
After any sinus operation, major bleeding, vision change, severe headache, clear drainage, fever with neck stiffness, neurologic change, or difficulty breathing requires urgent or emergency assessment.
An online form or routine appointment request is not an emergency service. For emergency symptoms, use emergency services rather than the routine form.
Medical review
This page is a patient-education resource reviewed by the responsible Norelle Health clinician before publication. It does not replace an in-person evaluation. If symptoms are severe or rapidly worsening, seek immediate medical care.
Specialists who perform revision sinus surgery

Dr. Adrian Ong
MD
Board-Certified Facial Plastic & Reconstructive and Head & Neck Surgeon
Dr. Adrian Ong is a board-certified surgeon who practices exclusively on the face, head, and neck, with expertise spanning rhinoplasty, sinus surgery, facial trauma, reconstruction, and sleep surgery.
- Functional and aesthetic rhinoplasty (including revision)
- Sinus surgery and complex revision sinus surgery
- Facial trauma and nasal fractures
- Head and neck cancer surgery and microvascular reconstruction
Also caring for this area


Not sure who to see? Our patient coordination team can help match you with the right specialist.
(212) 444-8006Frequently Asked Questions
Candidacy requires prior operative notes, imaging files, pathology, medication history, and a fresh endoscopic examination. The evaluation should separate persistent sinus disease from migraine, rhinitis, neuropathic pain, dental disease, or other explanations for ongoing symptoms.
The operation is individualized to distorted anatomy and the identified failure mechanism. It may address scarring, retained partitions, blocked frontal or sphenoid pathways, recurrent polyps, mucoceles, or other defined disease, often with navigation.
Alternatives may include optimized topical delivery, biologic treatment, management of asthma, AERD, or allergy, dental care, headache referral, observation, or a targeted rather than broad revision.
Recovery may resemble primary sinus surgery but varies with extent, scarring, and reconstruction. Frequent early follow-up, debridement, and long-term inflammatory control can be particularly important.
Clinical References
These independent resources from medical and professional organizations offer further reading. They are provided for general education and do not replace a consultation with a clinician.
Related Conditions

1 of 4 · Chronic Sinusitis
Related Procedures

1 of 4 · Endoscopic Sinus Surgery
Request a consultation about revision sinus surgery
Schedule a consultation with our team to discuss whether this procedure is the right option for you.